

Emergency situations demand swift action; obtaining IV access can be the difference between life and death. However, the process is fraught with difficulty, especially in patients with compromised vascular access due to dehydration, trauma, shock, obesity, or IV drug use. We introduce a practical algorithm specifically designed for IV access in emergency settings to streamline the decision-making process and enhance clinical outcomes. These algorithms are step-by-step guides that address initial site selection, techniques for difficult IV access, use of ultrasound-guided venipuncture, and alternative access methods such as IO infusion. It is intended to serve as a practical tool for clinicians, reducing the time to achieve access and improving patient care.
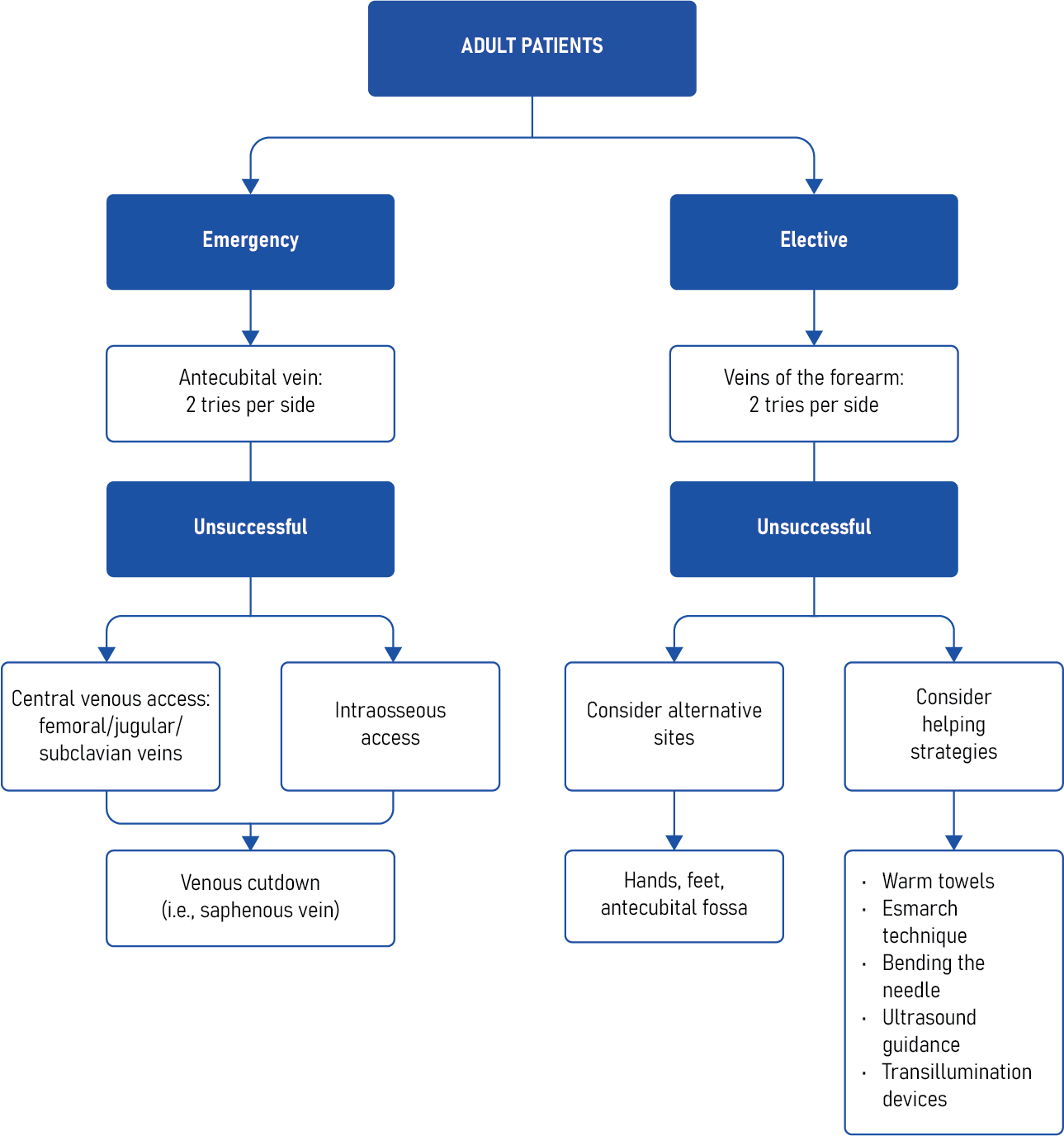
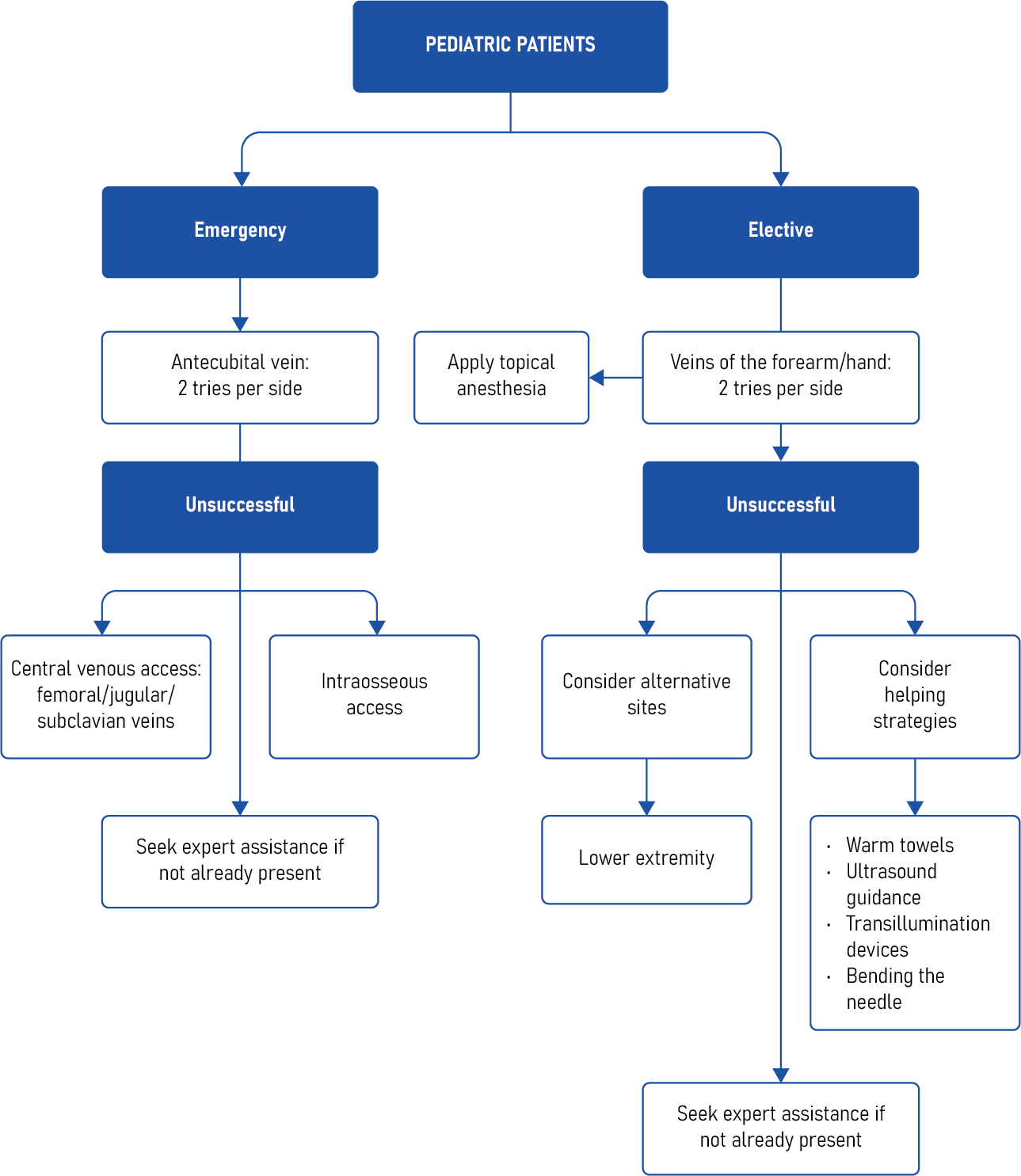
These algorithms emphasize a systematic approach, starting with the least invasive methods and progressing to more advanced techniques if initial attempts fail. They consider patient-specific factors and encourage clinicians to use clinical judgment and patient assessment to guide their choice of technique.
Clinical updates
- Vallentin et al. (New England Journal of Medicine, 2025) randomized 1479 adults with nontraumatic out-of-hospital cardiac arrest to initial intraosseous (IO) versus intravenous (IV) access and found no significant difference in sustained return of spontaneous circulation, 30-day survival, or favorable neurologic outcome. Although IO access achieved higher first- or second-attempt success, time to successful access and time to epinephrine were similar, and outcomes did not differ between humeral and tibial IO sites. These data suggest that in emergency cardiac arrest settings, clinicians may prioritize the fastest achievable route (IO or IV) without expecting differences in survival or neurologic outcomes.
Reference: Vallentin MF et al. Intraosseous or Intravenous Vascular Access for Out-of-Hospital Cardiac Arrest. N Engl J Med. 2025;392:349-360.
- Struck et al. (International Journal of Emergency Medicine, 2025) present the first German national S1 guideline specifically addressing vascular access in the resuscitation room, recommending that at least two large-bore peripheral IVs be established immediately, with rapid transition to intraosseous access in life-threatening situations or cardiac arrest when IV access fails. The guideline emphasizes ultrasound guidance for difficult peripheral access, central venous catheter (CVC), and arterial line placement; prioritizing IO over delayed IV in arrest; allowing peripheral vasopressor infusion under controlled conditions; and avoiding delays in critical imaging for CVC or arterial placement in stable patients. It also provides scenario-specific recommendations, including early arterial monitoring in critically ill patients, structured confirmation of catheter position, and strict fixation and documentation standards to reduce mechanical complications.
Reference: Struck MF et al. Vascular access for initial treatment of adult emergency patients in the resuscitation room: short summary of recommendations from the German national S1 guideline. Int J Emerg Med. 2025;18:187.












