
Explore NYSORA knowledge base for free:
Explore NYSORA knowledge base for free:


Complete learning material for your FIPP Exam on your mobile phone and tablet!




A recent study by Hallo-Carrasco et al. highlights the potential dangers of gadolinium-based contrast media (GCM) in interventional pain medicine. This research, published in Regional Anesthesia & Pain Medicine (2024), investigates adverse events linked to using GCM during spine procedures where inadvertent intrathecal administration is a risk. Here’s a comprehensive look at the findings, implications, and best practices surrounding GCM use in these procedures. Overview of gadolinium-based contrast media (GCM) Gadolinium-based contrast agents are an alternative for patients with documented allergies to iodinated contrast media (ICM). While traditionally safer for imaging, GCM carries specific risks: Toxicity risks: Gadolinium ions (Gd3+) are inherently toxic; chelating agents stabilize the compound and reduce these risks. Neurotoxicity: When inadvertently injected into the intrathecal (spinal) space, GCM can cause severe neurotoxic effects. Brain retention: There are concerns about gadolinium deposits in brain tissues following repeated exposure. Key findings Conducted via a retrospective review of medical records, the study investigated 508 patients who received GCM for spine-related procedures between 2019 and 2022. Here’s what was uncovered: Adverse event rate: 23 patients (3.3%) experienced adverse events potentially related to GCM. Common symptoms included severe pain, dizziness, headache, and, in one case, multifocal stroke. Patient demographics: A significant majority of patients were white females with a mean age of 67.55 years. Indications for GCM use: The predominant reason for using GCM was a documented iodine-related allergy. However, only 1% of these cases involved high-risk allergy reactions that could justify substituting ICM. Severity of adverse events: While most were manageable, some cases required hospitalization. The study documented one severe incident of stroke following GCM administration. Adverse reactions and symptoms Adverse effects following inadvertent intrathecal injection of GCM included: Severe pain: Reported within days of the procedure, sometimes requiring hospitalization. Headaches: Particularly postural headaches, which align with findings from other […]

Cervical disc herniation is a common condition that can cause significant pain, particularly when it leads to radicular pain. This article provides an in-depth look at a case of cervical hernia with radicular pain, detailing the diagnosis, treatment, and outcome. The focus will be on the Percutaneous Laser Disc Decompression (PLDD) procedure, a minimally invasive treatment option for patients with disc herniation who have not responded to conservative therapy. Case presentation A 41-year-old woman presented with cervical pain radiating to her left upper limb. The pain was aggravated by physical activities, including CrossFit, and was described as persistent, with shock-like sensations, pins and needles, and burning feelings. Pain intensity: Baseline pain was measured at 4/10 on the Numerical Rating Scale (NRS), peaking at 8/10 during episodes of exertion. Neurological evaluation: A detailed physical examination confirmed radicular pain following the C7 nerve root dermatome. Diagnosis Medical history and symptoms The patient reported no prior medical conditions but engaged in frequent high-intensity exercises, which may have contributed to the worsening of symptoms. The pain was consistent with radiculopathy, a condition characterized by nerve irritation due to a herniated disc. Physical examination findings: The Spurling test, a diagnostic maneuver used to assess cervical nerve root compression, was positive. The test aggravated the patient’s neck pain and reproduced the arm pain, indicating C7 nerve root involvement. Imaging: Magnetic Resonance Imaging (MRI) revealed a C6-C7 posterior disc protrusion with mild left-sided uncovertebral arthrosis, moderately narrowing the neural foramen. Final diagnosis The patient was diagnosed with cervical radiculopathy, specifically brachial plexus root pain caused by the C6-C7 disc herniation. This type of pain results from compression or irritation of the cervical nerve roots, often leading to pain that radiates down the arm. Treatment: Percutaneous Laser Disc Decompression (PLDD) What is PLDD? PLDD is a minimally invasive […]

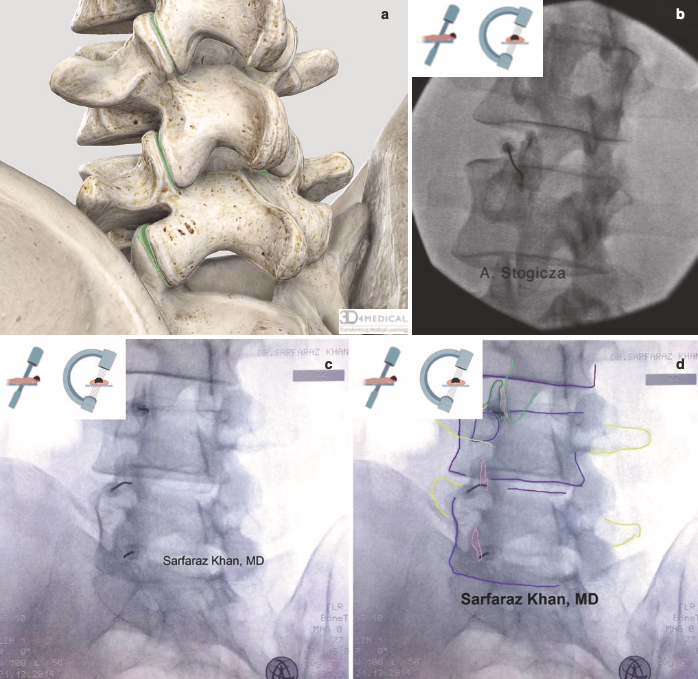
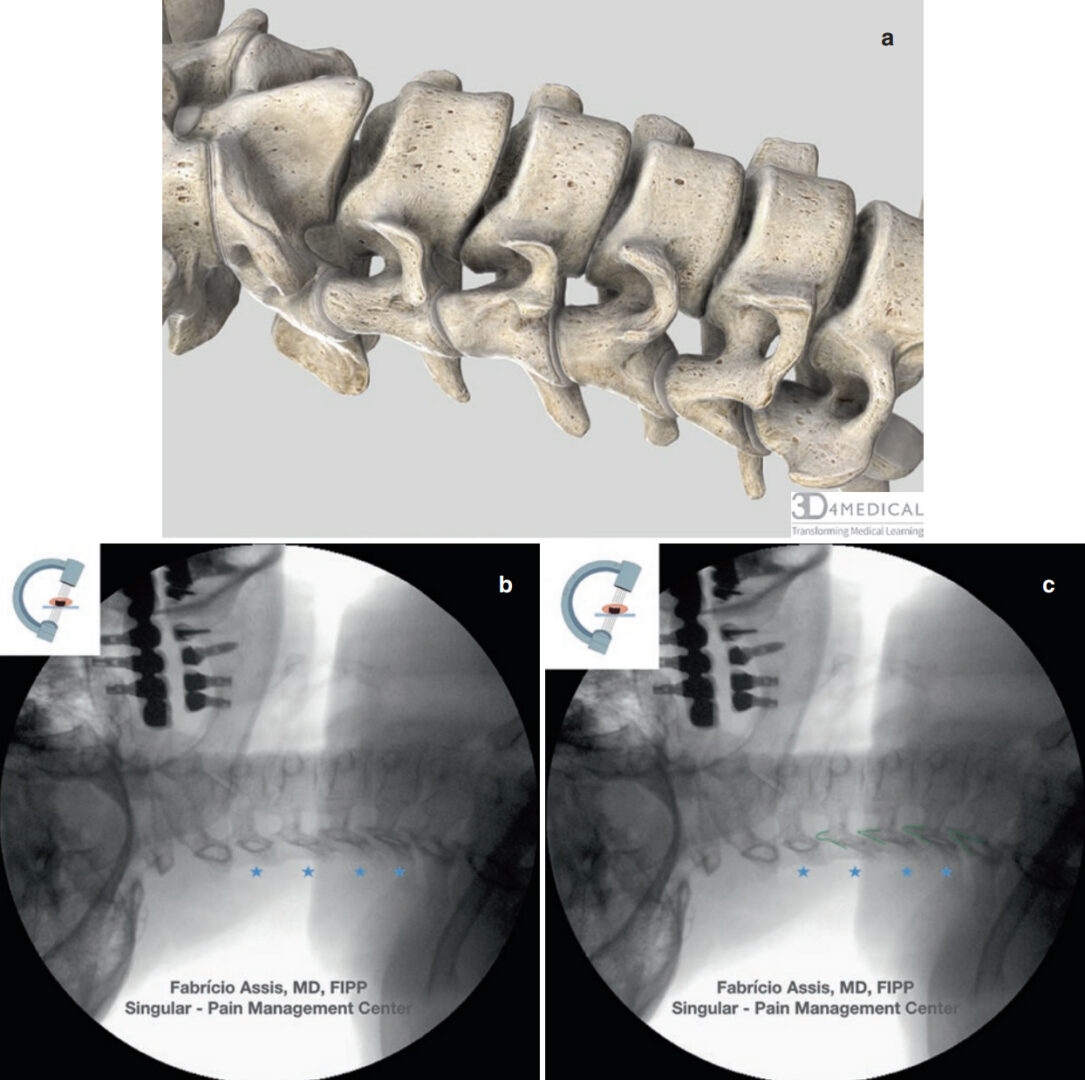
Cancer-related chronic pain is a debilitating condition that can significantly impact a patient’s quality of life. In this article, we will explore the case of a 55-year-old woman with cervical uterine malignancy and severe lower abdominal and pelvic pain. We will focus on her diagnosis, pain management, and the use of a superior hypogastric plexus neurolytic block to alleviate her chronic pain. This procedure offers a targeted approach for managing pain associated with pelvic malignancies. Case presentation A 55-year-old woman presented with persistent lower abdominal and pelvic pain. She had been diagnosed with moderately differentiated non-keratinizing squamous cell carcinoma of the uterine cervix six months prior. Despite receiving extensive chemotherapy and radiotherapy, her pain had escalated, becoming a significant challenge in her treatment journey. Diagnosis: Cervical uterine malignancy. Previous treatments: 5 sessions of chemotherapy 20 sessions of radiotherapy Pain characteristics Type: Severe, constant, with episodes of shooting, stabbing, and pressure-like sensations. Location: Lower abdomen and pelvis. Intensity: Baseline pain was rated at 7-8/10 on the Numerical Rating Scale (NRS), with peaks reaching 10/10 during episodes of excruciating pain. Duration: Episodes lasting for several seconds occurred multiple times per day, severely impacting her quality of life. Current pain management The patient’s pain was being managed with a multimodal approach, including: Gabapentin: 600 mg orally every eight hours. Duloxetine: 60 mg orally once daily. Methadone: 5 mg orally every eight hours. Paracetamol: 1000 mg orally every eight hours. Despite this regimen, her pain remained challenging to control, particularly the breakthrough episodes, which were unresponsive to conventional pain medications. Physical examination and imaging Physical exam: Revealed deep tenderness in the lower abdomen with organomegaly. Neurological examination of the legs was normal. MRI findings: Showed a large mass in the lower uterine cervix and upper vagina, with additional masses identified in the iliac, para-aortic, […]

A 59-year-old man, who has a history of celiac disease, presented with chronic left-hand pain after a wrist fracture from a traffic accident one year ago. The initial treatment for the fracture involved closed reduction, followed by surgical fixation. Unfortunately, the first surgical procedure led to a wound infection, which required further intervention through surgical debridement. Despite undergoing a second surgery, the patient has been suffering from persistent neuropathic pain in the left hand. This pain has progressively worsened over time, occasionally extending into the forearm and arm, and has been accompanied by intermittent episodes of discoloration and swelling in the affected areas. For pain management, the patient has been following a regimen of graded motor imagery and taking pregabalin (75 mg PO every 12 hours). The nature of the pain is persistent with intense episodes, scoring a baseline of 5 on the Numeric Rating Scale (NRS) and peaking at 8. Additionally, the patient has developed post-traumatic stress disorder (PTSD) following the traumatic experience and its subsequent complications. Physical examination Allodynia with mild trophic changes and erythema over the left hand and wrist. No dystonia was noted. Blood investigation Blood tests did not show leukocytosis or raised immune markers. Diagnosis The patient was diagnosed with complex regional pain syndrome (CRPS) of the left upper limb. CRPS is characterized by excessive, prolonged pain and inflammation following an injury to an arm or leg. Symptoms of CRPS include spontaneous pain, hyperalgesia, allodynia, changes in skin color, temperature, swelling in the affected limb, and alterations in skin texture. Read more about the treatment, patient outcome, and other case studies in the Pain Rx App. Click HERE and get the ultimate app for fluoroscopy-guided pain treatments

We are excited to share thrilling news with our community! NYSORA launches a new INTERVENTIONAL PAIN mobile app! With state-of-the-art, highly practical material from Springer’s best selling book “Interventional Pain: A Step-by-Step Guide for the FIPP Exam”, it’s a must-have for practitioners focusing on fluoroscopy-guided pain procedures. Read more about this great app here: https://www.nysora.com/nysora-interventional-pain-app/! The image-driven interventional pain procedures APP is created by the key opinion leaders with years of experience. With this app you will have instantaneous access to: Interventional Pain Procedures on the GO; Standardized Fluoroscopy-Guided Interventional Pain Procedures; Complete learning material for FIPP Exam on your mobile; Evidence-based recommendations asked at FIPP Exam; Tips on how to obtain the best images.. and much more! Download NYSORA’s Interventional Pain App on the buttons down below and start with your 7 days free trial!

NYSORA launches NEW Interventional Pain App by Springer, published by the world’s top experts on Interventional Chronic Pain management. We are excited to share thrilling news with our community! NYSORA has launched a new mobile app – Interventional Pain on July 19th, 2021. This state of the art, highly practical material from Springer’s best selling book “Interventional Pain : A Step-by-Step Guide for the FIPP Exam” by Springer Nature, is a must-have for practitioners with focus on fluoroscopy-guided pain procedures. Why should you get this APP? The image-driven interventional pain procedures APP is created by the key opinion leaders with years of experience. With this app you will have instantaneous access to: Interventional Pain Procedures on the GO; Standardized Fluoroscopy-Guided Interventional Pain Procedures; Complete learning material for FIPP Exam on your mobile; Evidence-based recommendations asked at FIPP Exam; Tips on how to obtain best images; Amazing mnemonics for remembering tips for success and complications; Best resource for both examinees and examiners; Improves patient care and safety; Fluoroscopic guidance for everything from cervical spine interventions, to sacroiliac and facet injections, to radiofrequency ablations. The newest edition, thoroughly updated with latest recommendations that cover the entire therapeutic area applicable to Fluoroscopic-guided Interventional Pain Medicine. NYSORA’s lead, Dr. Hadzic points out that this app is the single best resource featuring all standardized and evidence-based interventions in the practice of interventional pain medicine. Importantly, the app features clear guidance to diagnostic and therapeutic evidence-based recommendations, and it is the single best resource for preparing for the FIPP examination, administered by the World Institute of Pain (WIP). “We are committed to continually expand the educational resources utilizing our 20 years experience of transferring knowledge. Our educational mobile learning platforms benefit thousands of students and professionals who use NYSORA apps. For this new APP, we listened […]
A recent study by Hallo-Carrasco et al. highlights the potential dangers of gadolinium-based contrast media (GCM) in interventional pain medicine. This research, published in Regional Anesthesia & Pain Medicine (2024), investigates adverse events linked to using GCM during spine procedures where inadvertent intrathecal administration is a risk. Here’s a comprehensive look at the findings, implications, and best practices surrounding GCM use in these procedures. Overview of gadolinium-based contrast media (GCM) Gadolinium-based contrast agents are an alternative for patients with documented allergies to iodinated contrast media (ICM). While traditionally safer for imaging, GCM carries specific risks: Toxicity risks: Gadolinium ions (Gd3+) are inherently toxic; chelating agents stabilize the compound and reduce these risks. Neurotoxicity: When inadvertently injected into the intrathecal (spinal) space, GCM can cause severe neurotoxic effects. Brain retention: There are concerns about gadolinium deposits in brain tissues following repeated exposure. Key findings Conducted via a retrospective review of medical records, the study investigated 508 patients who received GCM for spine-related procedures between 2019 and 2022. Here’s what was uncovered: Adverse event rate: 23 patients (3.3%) experienced adverse events potentially related to GCM. Common symptoms included severe pain, dizziness, headache, and, in one case, multifocal stroke. Patient demographics: A significant majority of patients were white females with a mean age of 67.55 years. Indications for GCM use: The predominant reason for using GCM was a documented iodine-related allergy. However, only 1% of these cases involved high-risk allergy reactions that could justify substituting ICM. Severity of adverse events: While most were manageable, some cases required hospitalization. The study documented one severe incident of stroke following GCM administration. Adverse reactions and symptoms Adverse effects following inadvertent intrathecal injection of GCM included: Severe pain: Reported within days of the procedure, sometimes requiring hospitalization. Headaches: Particularly postural headaches, which align with findings from other […]
Cervical disc herniation is a common condition that can cause significant pain, particularly when it leads to radicular pain. This article provides an in-depth look at a case of cervical hernia with radicular pain, detailing the diagnosis, treatment, and outcome. The focus will be on the Percutaneous Laser Disc Decompression (PLDD) procedure, a minimally invasive treatment option for patients with disc herniation who have not responded to conservative therapy. Case presentation A 41-year-old woman presented with cervical pain radiating to her left upper limb. The pain was aggravated by physical activities, including CrossFit, and was described as persistent, with shock-like sensations, pins and needles, and burning feelings. Pain intensity: Baseline pain was measured at 4/10 on the Numerical Rating Scale (NRS), peaking at 8/10 during episodes of exertion. Neurological evaluation: A detailed physical examination confirmed radicular pain following the C7 nerve root dermatome. Diagnosis Medical history and symptoms The patient reported no prior medical conditions but engaged in frequent high-intensity exercises, which may have contributed to the worsening of symptoms. The pain was consistent with radiculopathy, a condition characterized by nerve irritation due to a herniated disc. Physical examination findings: The Spurling test, a diagnostic maneuver used to assess cervical nerve root compression, was positive. The test aggravated the patient’s neck pain and reproduced the arm pain, indicating C7 nerve root involvement. Imaging: Magnetic Resonance Imaging (MRI) revealed a C6-C7 posterior disc protrusion with mild left-sided uncovertebral arthrosis, moderately narrowing the neural foramen. Final diagnosis The patient was diagnosed with cervical radiculopathy, specifically brachial plexus root pain caused by the C6-C7 disc herniation. This type of pain results from compression or irritation of the cervical nerve roots, often leading to pain that radiates down the arm. Treatment: Percutaneous Laser Disc Decompression (PLDD) What is PLDD? PLDD is a minimally invasive […]
Cancer-related chronic pain is a debilitating condition that can significantly impact a patient’s quality of life. In this article, we will explore the case of a 55-year-old woman with cervical uterine malignancy and severe lower abdominal and pelvic pain. We will focus on her diagnosis, pain management, and the use of a superior hypogastric plexus neurolytic block to alleviate her chronic pain. This procedure offers a targeted approach for managing pain associated with pelvic malignancies. Case presentation A 55-year-old woman presented with persistent lower abdominal and pelvic pain. She had been diagnosed with moderately differentiated non-keratinizing squamous cell carcinoma of the uterine cervix six months prior. Despite receiving extensive chemotherapy and radiotherapy, her pain had escalated, becoming a significant challenge in her treatment journey. Diagnosis: Cervical uterine malignancy. Previous treatments: 5 sessions of chemotherapy 20 sessions of radiotherapy Pain characteristics Type: Severe, constant, with episodes of shooting, stabbing, and pressure-like sensations. Location: Lower abdomen and pelvis. Intensity: Baseline pain was rated at 7-8/10 on the Numerical Rating Scale (NRS), with peaks reaching 10/10 during episodes of excruciating pain. Duration: Episodes lasting for several seconds occurred multiple times per day, severely impacting her quality of life. Current pain management The patient’s pain was being managed with a multimodal approach, including: Gabapentin: 600 mg orally every eight hours. Duloxetine: 60 mg orally once daily. Methadone: 5 mg orally every eight hours. Paracetamol: 1000 mg orally every eight hours. Despite this regimen, her pain remained challenging to control, particularly the breakthrough episodes, which were unresponsive to conventional pain medications. Physical examination and imaging Physical exam: Revealed deep tenderness in the lower abdomen with organomegaly. Neurological examination of the legs was normal. MRI findings: Showed a large mass in the lower uterine cervix and upper vagina, with additional masses identified in the iliac, para-aortic, […]
A 59-year-old man, who has a history of celiac disease, presented with chronic left-hand pain after a wrist fracture from a traffic accident one year ago. The initial treatment for the fracture involved closed reduction, followed by surgical fixation. Unfortunately, the first surgical procedure led to a wound infection, which required further intervention through surgical debridement. Despite undergoing a second surgery, the patient has been suffering from persistent neuropathic pain in the left hand. This pain has progressively worsened over time, occasionally extending into the forearm and arm, and has been accompanied by intermittent episodes of discoloration and swelling in the affected areas. For pain management, the patient has been following a regimen of graded motor imagery and taking pregabalin (75 mg PO every 12 hours). The nature of the pain is persistent with intense episodes, scoring a baseline of 5 on the Numeric Rating Scale (NRS) and peaking at 8. Additionally, the patient has developed post-traumatic stress disorder (PTSD) following the traumatic experience and its subsequent complications. Physical examination Allodynia with mild trophic changes and erythema over the left hand and wrist. No dystonia was noted. Blood investigation Blood tests did not show leukocytosis or raised immune markers. Diagnosis The patient was diagnosed with complex regional pain syndrome (CRPS) of the left upper limb. CRPS is characterized by excessive, prolonged pain and inflammation following an injury to an arm or leg. Symptoms of CRPS include spontaneous pain, hyperalgesia, allodynia, changes in skin color, temperature, swelling in the affected limb, and alterations in skin texture. Read more about the treatment, patient outcome, and other case studies in the Pain Rx App. Click HERE and get the ultimate app for fluoroscopy-guided pain treatments
We are excited to share thrilling news with our community! NYSORA launches a new INTERVENTIONAL PAIN mobile app! With state-of-the-art, highly practical material from Springer’s best selling book “Interventional Pain: A Step-by-Step Guide for the FIPP Exam”, it’s a must-have for practitioners focusing on fluoroscopy-guided pain procedures. Read more about this great app here: https://www.nysora.com/nysora-interventional-pain-app/! The image-driven interventional pain procedures APP is created by the key opinion leaders with years of experience. With this app you will have instantaneous access to: Interventional Pain Procedures on the GO; Standardized Fluoroscopy-Guided Interventional Pain Procedures; Complete learning material for FIPP Exam on your mobile; Evidence-based recommendations asked at FIPP Exam; Tips on how to obtain the best images.. and much more! Download NYSORA’s Interventional Pain App on the buttons down below and start with your 7 days free trial!
NYSORA launches NEW Interventional Pain App by Springer, published by the world’s top experts on Interventional Chronic Pain management. We are excited to share thrilling news with our community! NYSORA has launched a new mobile app – Interventional Pain on July 19th, 2021. This state of the art, highly practical material from Springer’s best selling book “Interventional Pain : A Step-by-Step Guide for the FIPP Exam” by Springer Nature, is a must-have for practitioners with focus on fluoroscopy-guided pain procedures. Why should you get this APP? The image-driven interventional pain procedures APP is created by the key opinion leaders with years of experience. With this app you will have instantaneous access to: Interventional Pain Procedures on the GO; Standardized Fluoroscopy-Guided Interventional Pain Procedures; Complete learning material for FIPP Exam on your mobile; Evidence-based recommendations asked at FIPP Exam; Tips on how to obtain best images; Amazing mnemonics for remembering tips for success and complications; Best resource for both examinees and examiners; Improves patient care and safety; Fluoroscopic guidance for everything from cervical spine interventions, to sacroiliac and facet injections, to radiofrequency ablations. The newest edition, thoroughly updated with latest recommendations that cover the entire therapeutic area applicable to Fluoroscopic-guided Interventional Pain Medicine. NYSORA’s lead, Dr. Hadzic points out that this app is the single best resource featuring all standardized and evidence-based interventions in the practice of interventional pain medicine. Importantly, the app features clear guidance to diagnostic and therapeutic evidence-based recommendations, and it is the single best resource for preparing for the FIPP examination, administered by the World Institute of Pain (WIP). “We are committed to continually expand the educational resources utilizing our 20 years experience of transferring knowledge. Our educational mobile learning platforms benefit thousands of students and professionals who use NYSORA apps. For this new APP, we listened […]



