INTRODUCTION
Patients with coexisting systemic disease may be at a higher risk for specific perioperative complications related to surgery and anesthesia. Regional anesthesia is often thought of as being particularly beneficial in patients. However, the physiologic changes that occur with some regional anesthesia techniques must be understood and viewed within the context of an individual patient’s pathophysiology so that the technique used provides maximum patient benefit and reduces the risk of complications. This chapter focuses on the pathophysiology of systemic diseases frequently encountered by the regional anesthesiologist and discusses the interplay between common regional anesthesia techniques and patient disease.
PULMONARY DISEASE
Surgical patients with coexisting pulmonary impairment are at risk for intraoperative or postoperative pulmonary complications, regardless of anesthetic technique. A growing body of evidence suggests that regional anesthesia may be associated with improved pulmonary outcomes compared with general anesthesia. However, regional anesthetic block may carry risks in some patients. A thorough understanding of respiratory physiology and the implications of regional anesthetic techniques is crucial to the safe and effective use of regional anesthesia in these patients.
Epidural & Spinal Anesthesia
Most of the pulmonary effects of neuraxial anesthesia are due to motor block of the intercostal and abdominal musculature. If significant systemic uptake of local anesthetic occurs, some central and direct myoneural respiratory depression can also be seen, although this plays a minor role overall. Since neuraxial anesthesia produces a “differential” block of motor, sensory, and autonomic fibers, the degree to which respiratory function is impaired depends on the relative extent of segmental motor block. Using dilute concentrations of epidural local anesthetic may provide adequate sensory block as high as the cervical levels, while sparing the motor function of the respiratory muscles in the lower somatic segments. Diaphragmatic paralysis (phrenic nerve block, C3–C5) in the absence of total spinal anesthesia does not occur with neuraxial block, since even a sensory block as high as C3 will only produce a motor block at approximately T1 through T3. Apnea following high neuraxial anesthesia is most likely precipitated by brainstem hypoperfusion as a result of hypotension and unlikely to be related to phrenic nerve block. Spontaneous respiration returns following adequate volume resuscitation and/or vasopressor therapy.
NYSORA Tips
- Apnea associated with a high spinal anesthetic is most often related to hypotension and hypoperfusion of the brainstem, rather than motor block of the nerve roots supplying the phrenic nerve (C3–5).
- Supporting ventilation while maintaining the blood pressure with fluids and vasopressor therapy is the key resuscitative strategy.
With a high level of epidural or spinal anesthesia, the chest wall musculature and intercostal muscles may become impaired. This may even result in altered chest wall motion during spontaneous respiration. During high neuraxial anesthesia, the more compliant chest wall is retracted during inspiration and may actually display paradoxical rib cage motion. Some, however, have found that epidural block to sensory levels of T6 or even T1 may increase the contribution that chest wall expansion makes to tidal volume. This may be explained by an incomplete motor block of high intercostal muscles or the compensatory role played by the “accessory” muscles of respira-tion, such as the anterior and middle scalene muscles.
Lumbar epidural anesthesia does not affect resting minute ventilation, tidal volume, or respiratory rate. Likewise, functional residual capacity (FRC) and closing capacity appear to be relatively unchanged during lumbar epidural anesthesia. Effort-dependent tests of respiratory function, such as forced expiratory volume in one second (FEV1), forced vital capacity, and peak expiratory flow, do exhibit modest decreases in the setting of lumbar epidural block, reflecting the reliance of these indices on intercostal and abdominal musculature. This decrease in pulmonary function increases proportionally as the block progresses in a cephalad fashion from lower to upper lumbar regions.
Thoracic epidural anesthesia has no effect on minute ventilation, tidal volume, or respiratory rate but does result in a modest decrease in vital capacity (VC), FEV1, total lung capac-ity, and maximal midexpiratory flow rate (Table 1). Even low cervical/high thoracic epidural anesthesia (C4–T9) in patients with severe chronic obstructive pulmonary disease (COPD) undergoing breast surgery produces only a very mild decrease in FEV1. One volunteer study found that high thoracic epidural anesthesia (T1 sensory level) led to an increase in FRC of approximately 15% with no change in tidal volume or respiratory rate. This somewhat surprising finding may be explained by two mechanisms offered by the investigators. First, most volunteers exhibited a decrease in intrathoracic blood volume, a physiologic phenomenon confirmed by Arndt and colleagues. Second, the study also found that the end-expiratory position of the diaphragm was shifted caudally, which may be related to a relative increase in diaphragmatic tonic activity or a reduction in intra-abdominal pressure.
TABLE 1. The eect of epidural anesthesia on respirator volumes and mechanics.
| VC | TLC | FRC | VT | RR | MV | FEV1 | FVC | PEF | |
|---|---|---|---|---|---|---|---|---|---|
| LEA | ↔ | ↔ | ↔ | ↔ | ↔ | ↔ | ↓ | ↓ | ↓ |
| TEA | ↓ | ↓ | ↑ | ↔ | ↔ | ↔ | ↓ | ↓ | ↓ |
Cervical epidural anesthesia reduces the VC and FEV1 to a degree similar to that of high thoracic epidurals that extend to lower cervical levels. Studies on healthy patients have demon-strated a 15–30% reduction in VC and FEV1 with cervical epidurals (sensory block to C2) that varied by level and local anesthetic concentration.
The ventilatory response to hypercarbia and hypoxia is preserved with neuraxial anesthesia. Partial pressures of both oxygen (Po2) and carbon dioxide (Pco2) are essentially unchanged during epidural or spinal anesthesia. In addition, bronchomotor tone is not altered to any significant degree, despite theoretical concerns of bronchoconstriction secondary to sympatholysis. Indeed, epidural anesthesia has been used successfully in high-risk patients with COPD and asthma undergoing abdominal operations.
Neuraxial anesthesia has been shown in a number of settings to lead to reduced postoperative pulmonary complications compared with general anesthesia. Perlas and colleagues reported an association between spinal anesthesia and lower 30-day mortality. The reasons behind this are probably multifactorial, owing in part to superior analgesia, reduced diaphragmatic impairment, altered stress response, and a decreased incidence of postoperative hypoxemia. Epidural anesthesia provides superior pain control over general anesthesia with postoperative opioids for abdominal and thoracic surgery, which leads to reduced splinting, a more effective cough mechanism, and preserved postoperative lung volumes, includ-ing FRC and VC. One study directly comparing epidural and general anesthesia in high-risk patients concluded that overall outcomes, including the need for prolonged postoperative ventilation, were improved with the regional technique. Another trial in patients undergoing lower limb vascular surgery reported a greater than 50% reduction in the incidence of respiratory failure in the group randomized to epidural anesthesia.
Patients undergoing repair of hip fractures also benefits from regional anesthesia. Neuman et al. compared neuraxial versus general anesthesia for hip fracture repair in over 18,000 patients and found a 25% reduction in pulmonary complications in those who received neuraxial techniques. A meta-analysis of 141 randomized trials (including over 9000 patients) comparing regional and general anesthesia for hip surgery showed a risk reduction for pulmonary embolism, pneumonia, and respiratory depression of 55%, 39%, and 59%, respectively, with the regional anesthesia. Interestingly, these outcomes were unchanged regardless of whether neuraxial anesthesia was continued into the postoperative period, illustrating that the beneficial effect of epidural and spinal anesthesia on pulmonary physiology occurs, at least in part, at the time of surgical insult.
Brachial Plexus Block
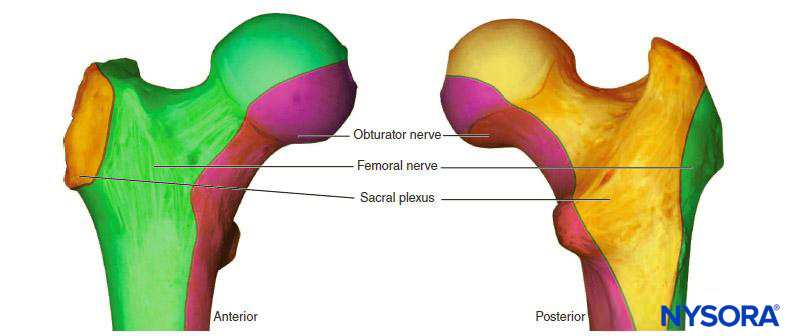
In the absence of rare complications such as pneumothorax, any alterations in respiratory mechanics seen with brachial plexus block are due primarily to phrenic nerve block and hemidiaphragmatic paralysis (Figure 1). This has been shown to occur in 100% of patients receiving interscalene block when performed without ultrasound guidance and using between 34 and 52 mL of local anesthetic. When diaphragmatic paresis occurs, there is an associated 27% reduction in both FVC and FEV1. While the clinical significance of this reduction in healthy patients is not entirely clear, it may be useful to risk-stratify patients about to undergo interscalene blocks as one would a patient undergoing lung resection. In other words, ask the question, “Will this patient tolerate a periopera-tive FEV1 reduction of 27%?”

FIGURE 48-1. Upright chest radiograph of a patient who underwent a right interscalene brachial plexus block. Note the elevated right hemidiaphragm.
Some investigators have attempted to reduce the incidence of phrenic nerve palsy by decreasing the volume of local anesthetic. However, Sinha et al. found no reduction in the incidence of hemidiaphragmatic paresis (as measured by ultrasound) when the volume of ropivacaine 0.5% was reduced from 20 mL to 10 mL. Others have reported that reducing volume to 5 mL decreases the incidence by 45%–50% and results in a significantly reduced impairment of FEV1 and peak expiratory flow (PEF). Low volumes of local anesthetic are no guarantee of preservation of phrenic nerve function. Clinically significant respiratory compromise requiring tracheal intubation has been reported following an interscalene brachial plexus block using a volume of 3 mL of 2% mepivacaine.
NYSORA Tips
- Interscalene block with low (≤ 5 mL) volumes of local anesthetic may reduce but not eliminate the risk of phrenic block and diaphragmatic paresis.
- Therefore, interscalene brachial plexus block should be avoided in patients who could not tolerated a 25% decrease in respiratory function.
The risk of phrenic nerve block decreases as one moves more distally along the plexus. The axillary approach to the brachial plexus has no effect on diaphragm function and presents a good choice for those patients with marginal pulmonary reserve (ie, cannot tolerate a 27% reduction in lung function). On the other hand, the supraclavicular block has been traditionally associated with a 50%–67% incidence of hemidiaphragmatic paralysis, although recent studies have shown that with ultrasound guidance the incidence can be as low as zero. The infraclavicular approach is probably suffi-ciently distant from the course of the phrenic nerve so as to spare the diaphragm,40,41 although there are case reports of phrenic nerve involvement.42,43 These discrepancies probably relate to the dif-ferent approaches to the infraclavicular block—for instance the “coracoid block” is performed with a relatively lateral or distal puncture site, whereas the vertical infraclavicular block begins at a more medial location. There may also be some anatomic variations in the course of the phrenic nerve, such as an acces-sory phrenic nerve, which would make it more susceptible to block at more distal levels of the brachial plexus.44
Although the infraclavicular or axillary blocks may be desirable for their relative pulmonary-sparing profiles, they carry the disadvantage of providing incomplete anesthesia for the shoulder and require higher degree of expertise to perform. However, creative solu-tions have been employed to get around this issue. Martinez and colleagues combined an infraclavicular block with a supra-scapular nerve block for emergent humeral head surgery in a patient with acute asthma and a baseline FEV1 of 1.13 L (32% predicted). The combination of axillary and suprascapular blocks has also been suggested as an alternative to interscalene block. Therefore, a carefully considered selection of peripheral nerve blocks can provide complete anesthesia of the upper limb while avoiding respiratory complications in patients with pul-monary disease.
Continuous brachial plexus blocks with perineural catheters can extend the benefits of plexus block into the postoperative period and reduce postoperative pain, oral opioid requirements and their side effects, and sleep disturbances after shoulder surgery. However, there have been reports of com-plications attributed to the prolonged phrenic nerve paresis that can occur with this technique. These have included chest pain, atelectasis, pleural effusion, and dyspnea. This is of particular concern because many patients are being discharged home with catheters and may not have access to timely intervention should these complications arise. On the other hand, the degree of clinically significant respiratory impairment with continuous interscalene block varies among patients, and, in fact, interscalene block may be well tolerated, especially if using relatively dilute concentrations of local anesthetic that provide only a partial phrenic nerve block. Maurer and associates reported a case of a patient with no preexisting pulmonary disease who underwent bilateral shoulder arthroplasty under combined bilateral continuous interscalene block and general anesthesia. Postoperative analgesia was maintained in the hospital for 72 hours via the catheters using infusions of 7 mL/h of 0.2% ropivacaine for each side (total 14 mL/h). Despite a marked postoperative reduction in FVC (60%) from baseline as well as sonographic evidence of diaphragmatic impairment, the patient had an uneventful postoperative course (with excellent analgesia) and good recovery. This anecdotal example illustrates that the clinical significance of phrenic paresis in patients with good respiratory function is questionable. Regard-less, the use of continuous brachial plexus techniques should be carefully considered in patients with preexisting pulmonary dis-ease, especially if they are to be discharged home with the catheters in situ. Other complications that may have pulmonary implications include interpleural, epidural, or even intrathecal catheter migration and irritation of the phrenic nerve.
NYSORA Tips
- The clinical consequences of phrenic in patients with normal respiratory function are typically asymptomatic or mild.
- The use of continuous brachial plexus techniques should be carefully considered in patients with preexisting sig-nificant pulmonary disease.
- When indicated, catheter can be bolus with a small amount of short-acting local anesthetic (eg, 2% chloro-procaine 5 ml) to evaluate the effect on the respiratory function before using long-acting local anesthetics.
- In symptomatic patients with indwelling catheter, an injection of 0.9% NaCl can shorten the duration of phrenic (and brachial plexus) block (“washout”).
Paravertebral & Intercostal Nerve Blocks
Several studies have investigated the effects of paravertebral and intercostal blocks on pulmonary function in patients with rib fractures or those undergoing thoracotomy. Intercostal block-ade has been shown to improve arterial oxygen saturation (Sao2) and peak expiratory flow rate (PEFR) in patients with trau-matic rib fractures associated with severe pain. In addition to improved pulmonary function, some studies found significantly improved pain control and shortened hospital length of stay following intercostal catheter placement. Likewise, Kar-makar and co-investigators found that continuous paravertebral block over a period of four days in patients with multiple fractured ribs led to significant improvement in respiratory rate, FVC, PEFR, Sao2, and the ratio of partial pressure of oxygen to fraction of inspired oxygen (Pao2:Fio2). These findings are probably related to the favorable effect of analgesia on respiratory efforts by the patient and improved respiratory mechanics, facilitating weaning from ventilator support and return to activities of daily living in patients who were otherwise in distress from their injuries.
Paravertebral blocks are effective for the management of pain following thoracotomy and can significantly improve postoperative spirometry. One review of 55 randomized, controlled trials of analgesic techniques following posterolateral thoracotomy revealed that paravertebral block was the method that best preserved pulmonary function compared with either intercostal or epidural analgesia. The combined results showed an average preservation of approximately 75% of pre-operative pulmonary function when paravertebral analgesia was used versus 55% for both intercostal and epidural analgesia. In addition, Davies et al showed that even when comparable analgesia was obtained with paravertebral block and thoracic epidural, the side effect profile with paravertebral block was significantly better, resulting in fewer pulmonary complications and less hypotension, nausea, and urinary retention. It is unclear why paravertebral block might result in improved PEFR and SaO2 compared with epidural analgesia in this and other studies, but it may be related to the increased utilization of opioids, a higher incidence of nausea and vomiting, and the presence of bilateral intercostal muscle block (and therefore diminished chest wall mobility) in the epidural cohorts.
NYSORA Tips
- Paravertebral or intercostal block provides excellent analgesia following both rib fracture and thoracotomy.
- These blocks also result in improved spirometry and pulmonary outcomes.
Pulmonary Complications Not Related to Conduction block
Pulmonary complications related to the use of regional anesthetic techniques fall into two categories. The first is those related directly or indirectly to the physiologic changes that occur with the block itself. Examples include atelectasis and pneumonia resulting from an inability to mobilize secretions. The second category comprises those that are independent of the effect of block, and although there are sporadic reports of rare complications such as pulmonary hemorrhage and chylothorax, the most common of these is pneumothorax. Not surprisingly, pneumothoraces occur most frequently when the puncture site overlies the pleura, and especially when per-forming supraclavicular and intercostal blocks. The overall reported incidence is low, but the actual numbers are likely to be underreported, since many pleural punctures will result in small pneumothoraces that resolve spontaneously. Refinements of previously published infraclavicular techniques based on MRI studies and the widespread use of ultrasound guidance may confer additional safety to these procedures, although is important to note that pneumothoraces have been reported with ultrasound-guided techniques, highlighting the fact that ultrasound guidance is an imperfect means of preventing adverse events.
RENAL DISEASE
Renal dysfunction is commonly present in the surgical population. Perioperative acute kidney injury accounts for approximately 50% of all patients requiring acute hemodialysis in the United States. Patients with chronic renal insufficiency frequently present for procedures such as the creation of vascular shunts and revascularization of the lower limbs. Regional anesthetic techniques are frequently ideal options to provide anesthesia for these patients and procedures.
Effect of Regional Anesthesia on Renal Function
The treatment of patients at risk for perioperative renal dysfunction should focus on two principles: avoiding nephrotoxic agents and maintaining kidney perfusion. Local anesthetics do not possess any nephrotoxic properties per se, and in fact the coadministration of procaine has been shown to mitigate some of the nephrotoxic effects of cisplatin in rats. Of greater relevance is the effect of anesthetic-induced hypotension on renal blood flow. The kidneys are capable of autoregulation over a wide variety of mean arterial pressures (approximately 80–180 mmHg) and maintain the glomerular filtration rate (GFR) by autonomous changes in renal vascular resistance. Below the so-called lower limit of autoregulation, the kidney begins to shut down its energy-dependent physiologic processes, and the GFR and urinary output fall as a result. Ultimately, if left unchecked, renal ischemia develops, especially in the sensitive renal medulla. Although neuraxial anesthesia and the concurrent sympathectomy can reduce mean arterial pressure (MAP), renal blood flow is often preserved. This is believed to reflect an increase in left ventricular stroke volume in response to the drop in systemic vascular resistance (SVR). Rooke and colleagues studied hemodynamic responses and abdominal organ perfusion (as measured by scintigraphy) in 15 patients undergoing lidocaine spinal anesthesia with a sensory block ranging from T1 to T10. Whereas the MAP and SVR fell on average by 33% and 26%, respectively, blood volume in the kidneys increased by approximately 10%. There may be limits to the degree of compensation afforded by cardiac output, however. One study using a primate model showed that although renal blood flow was minimally affected by T10 spinal anesthesia, it was significantly reduced by a T1 sensory block. This finding illustrates again that lumbar and low-thoracic levels of neuraxial anesthesia in patients with renal disease are well toler-ated physiologically and that significant changes do not begin to manifest until higher levels are achieved.
The renin–angiotensin system, which is initiated in the kidney in response to a reduction in renal perfusion, plays an important role in blood pressure homeostasis. It serves as a complementary humoral mechanism to the sympathetic ner-vous systems. Hopf and colleagues conducted a study to deter-mine if thoracic epidural anesthesia suppressed the renin response to induced hypotension. Plasma renin and vasopres-sin concentrations were measured before, during, and after a hypotensive challenge with nitroprusside in patients with and without thoracic epidural anesthesia (sensory levels T1 through T11). With an intact sympathetic nervous system (ie, no epidural), plasma renin levels doubled in response to the hypotensive challenge lasting 15 minutes. In contrast, there was no change in the renin concentration when hypotension was induced to the same MAP in the epidural cohort. This suggests that sympathetic fibers play a key role in the renin–angiotensin system and that thoracic epidural anesthesia interferes with the functional integrity of that system.
NYSORA Tips
- Lumbar and low-thoracic levels of neuraxial anesthesia significantly renal hemodynamics.
For obvious reasons, postoperative renal function is of fore-most concern when administering anesthesia for recipients of renal transplantation. Several studies have looked at the effect of general versus regional (or combined epidural/general) anes-thesia on postoperative renal function in this setting. While regional anesthesia has been shown to reduce the stress response to renal transplant surgery and improve postoperative pain control, anesthetic technique was not shown to have an effect on graft outcome in either adult or pediatric populations. Also, the choice of anesthetic technique for living donors was shown to be independent of recipient graft outcome. Other nontransplant outcomes data, including those from the large meta-analysis by Rodgers et al., indicate that regional anesthesia is associated with a lower risk of postoperative renal failure than general anesthesia. However, the authors cautioned that the confidence intervals were wide and were compatible with both no effect and a two-thirds risk reduction. Overall, it appears that a well-conducted regional anesthetic does not negatively affect perioperative kidney function or renal outcome com-pared with general anesthesia.
Considerations for Regional Anesthesia in Chronic Renal Failure
Patients with chronic renal failure often manifest a large number of pathophysiologic changes that may influence regional anesthetic care. These may include the presence of an anion-gap metabolic acidosis, electrolyte disturbances such as hyperkalemia, and coagulopathies due to uremia-induced platelet dysfunction. Plasma concentrations of local anesthetic following peripheral nerve blocks are often high enough to cause central nervous system (CNS) or cardiac toxicity in any patient, even when no obvious intravascular injection has occurred. This is probably dose-related when performing “high-volume blocks” such as plexus blocks. Some authors have recommended that dosages be adjusted in patients with chronic renal insufficiency based on observations of toxicity presumed to be related to concurrent acidosis or hyperkalemia. Indeed, experimental evidence suggests that acidemia decreases the protein binding of bupivacaine, thereby increasing the free fraction and risk of toxicity. In addition, it has been shown that hyperkalemia (5.4 vs 2.7 mEq/L) in dogs results in just half the dose of bupivacaine being required to induce cardiotoxicity. Interestingly, the potassium level had no effect on in the same animals. This is an ominous finding, as it suggests that the so-called safety margin of plasma levels between CNS and cardiac toxicity, which is already relatively narrow with bupivacaine, is even less reliable in the presence of hyperkalemia.
NYSORA Tips
- Acidemia and hyperkalemia decrease the protein binding of bupivacaine, thereby increasing the free fraction and the risk of toxicity.
- Patients with uremia may have higher plasma levels of local anesthetic following peripheral nerve block.
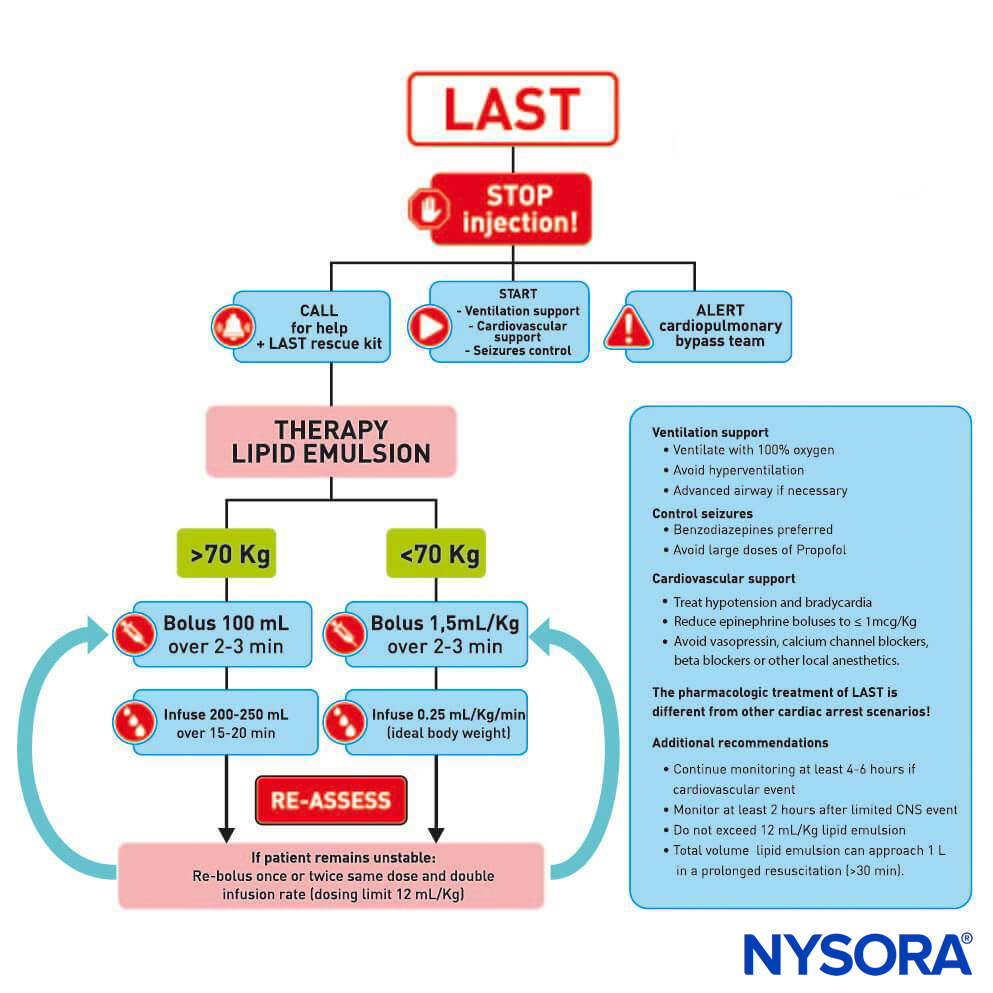
Even in the absence of acid–base or electrolyte disturbances, plasma levels of local anesthetics following peripheral nerve block are often higher in patients with chronic renal failure. The reason for this is not entirely clear but may relate to increased blood flow (and hence uptake at the injection site) due to the hyperdynamic circulation often seen in uremic patients. On the other hand, a1-acid glycoprotein (AAG) levels are increased in uremia and may lend a protective effect by binding more local anesthetic in the bloodstream. The increased levels of AAG also result in both a reduced free fraction available for hepatic metabolism and in a reduced volume of distribution. These two pharmacokinetic consequences appear to balance each other so that the serum half-life is not significantly changed. Hemodialysis is ineffective in removing lidocaine from plasma and therefore cannot be relied on to treat toxicity. However, lipid emulsion has been used successfully to treat both cardiovascular and neurologic systemic toxicity in patients with renal failure.
No significant difference exists between patients with chronic renal failure and healthy patients with respect to peripheral nerve block latency, duration, or quality. In one study of spinal anesthesia in patients with chronic renal failure versus healthy patients, Orko and associates found that block quality was similar but that both onset time and duration of the block were reduced in patients with uremia. The authors postulated a volume-contracted intrathecal space in uremic patients as a mechanism for the quicker onset, but the actual cause remains unclear. The shorter duration of sensory block may again be related to enhanced uptake in the setting of a hyperdynamic circulation. Uremic coagulopathy is characterized by a defect of platelet aggregation that is probably due to a toxic effect by uremic substances on the binding of fibrinogen to the platelet glycoprotein IIb/IIIa receptor. This often manifests in clinically appreciable bleeding, and at least one case of subarachnoid hematoma leading to paraplegia after a spinal anesthetic in a chronic renal failure patient has been published. Patients undergoing hemodialysis require intermittent anticoagulation and may present to the operating room with an unclear coagulation status. Care must be taken to delineate heparin or other anticoagulant regimens. Despite this platelet dysfunction, uremic patients are at higher risk for thrombotic events. One case of hypoxia following a brachial plexus block in a uremic patient was later found to be secondary to pulmonary embolism. The authors of the report suggested that a likely mechanism was the dislodgment of a preexisting thrombus from the proximal arm, facilitated by block-related manipulation and vasodilation of the upper extremity.
Several studies have compared anesthetic techniques for the creation of arteriovenous fistulae, a procedure that is common in patients with end-stage renal disease and is well suited to brachial plexus block. Some investigators have concluded that little difference exists in outcome among general, local, and brachial plexus anesthesia for this operation. Mouquet and colleagues specifically studied the effects of these three techniques on brachial artery blood flow and concluded that both general anesthesia and brachial plexus block improved blood flow through the fistula during surgery, whereas local infiltration did not. Several subsequent studies have shown increased vein diameter, increased rates of native fistula formation, increased fistula blood flow, and shorter maturation time when regional anesthesia is used, compared to either general or local anesthesia.
HEPATIC DISEASE
Liver injury or dysfunction can range from a mild, asymptomatic “transaminitis” to frank hepatic failure. There are many causes of liver disease, both acquired and congenital, but all manifest as either failure of parenchymal cell function (ie, acute and chronic hepatitis, cirrhosis) or cholestasis. Considerations for regional anesthesia in patients with liver disease include the potential for altered disposition and metabolism of local anesthetics, the effect of regional anesthesia on hepatic perfusion, and possible coagulopathy related to liver dysfunction.
Pharmacokinetics of Local Anesthetics in Liver Disease
Amide local anesthetics are metabolized in liver microsomes by the cytochrome P450 system. A decrease in microsomal function, as may be seen in acute or chronic liver disease, can lead to a reduction in biotransformation and clearance of these drugs, putting the patient at risk for local anesthetic toxicity. As with other drugs that are metabolized in the liver, the hepatic extraction ratio determines the relative importance of hepatic perfusion versus intrinsic enzyme activity in the overall clearance of the drug. For example, bupivacaine has a low extraction ratio (ie, its clearance is more sensitive to alterations in hepatic enzyme activity), whereas etidocaine exhibits a relatively high extraction ratio and depends on adequate liver perfusion for clearance. Lidocaine has an intermediate hepatic extraction ratio and therefore relies on both perfusion and enzymatic activity. Severe hepatic disease such as cirrhosis can affect both liver perfusion and intrinsic enzyme function. In this scenario, the clearance of all amide local anesthetics, regardless of their extraction ratio, is likely to be reduced. Because the volume of distribution of local anesthetics (and many other drugs) is increased in hepatic disease, the actual plasma levels may not differ significantly from healthy patients with a single dose, despite the diminished clearance. The altered distribution may be related to decreased levels of plasma AAG, which are reduced in proportion to the severity of liver disease. Clinically, it appears that single-dose peripheral nerve blocks with amide local anesthetics probably do not require a dosage adjustment in this population, whereas continuous infusions or repeated boluses have the potential to accumulate to toxic levels. This is supported by a study comparing plasma levels of levobupivacaine in patients undergoing hepatic resection or colorectal surgery who received epidural levobupivacaine by repeated bolus. Patients in the hepatic resection group were found to have significantly higher plasma levels, which correlated with indocyanine green clearance (a measure of hepatic function) and plasma bilirubin concentration.
The cytochrome P450 enzyme system is subject to induction or inhibition by a variety of drugs and dietary nutrients. This may play a role in the subsequent metabolism of amide local anesthetics. For example, substances that inhibit microsomal enzymes, such as cimetidine or grapefruit juice, may lead to an accumulation of local anesthetic, augmenting the risk of toxicity, especially in the setting of preexisting hepatic dysfunction.
Ester local anesthetics are cleared by plasma cholinesterases in the blood and liver. Severe hepatic disease may result in decreased levels of cholinesterase and result in prolonged plasma half-lives of esters such as procaine. On the other hand, red cell esterases remain intact during liver disease and are able to provide some hydrolytic function. Because plasma cholinesterase is extremely efficient, it is unlikely that an enzyme deficiency secondary to hepatic disease could impair the hydrolysis of ester-type local anesthetics to a degree sufficient to cause toxicity.
NYSORA Tips
- The pharmacokinetics of local anesthetics in patients with liver disease can be complex due to the decrease in protein production and drug metabolism.
- Single injection-dose peripheral nerve blocks with amide local anesthetics probably do not require a dosage adjustment in patients with hepatic disease.
Effect of Regional Anesthesia on Hepatic Blood Flow
The hepatic blood supply is unique in that it relies on both portal venous return and hepatic artery blood flow, which make up approximately 75% and 25% of the total flow, respectively. The regulation of hepatic blood flow is complex. The portal system is passive and not subject to autoregulation, whereas the hepatic artery can increase or decrease its contribution to flow in response to alterations in portal venous flow. The hepatic artery also autoregulates in response to MAP, in much the same way that cerebral or renal vessels do, but may rely on an intact sympathetic response.
General anesthesia has been shown to cause a decrease in hepatic blood flow, which may lead to ischemia and postoperative liver dysfunction. Less is known about the effects of regional anesthesia on hepatic perfusion. Grietz et al. performed a high epidural (block level T1 through T4) in 16 dogs and examined the effect on systemic and hepatic hemodynamics. MAP and portal venous flow were both reduced compared with control values, by 52% and 26%, respectively. In contrast, hepatic artery flow was unchanged, probably relating to a reduction in hepatic artery resistance of 51%. In addition, hepatic oxygen uptake was preserved through an increased oxygen extraction. Another study by Vagts and colleagues found that thoracic epidural anesthesia in anesthetized pigs was associated with decreased mean arterial blood pressure and hepatic artery blood flow but no change in hepatic oxygen delivery or uptake or tissue oxygen partial pressure compared with pigs receiving general anesthesia alone. Taken together, these findings should reassure the clinician that high neuraxial anesthesia may be well tolerated with respect to hepatic oxygenation, despite a modest reduction in MAP. Care should be taken to maintain cardiac output and perfusion pressure during anesthe-sia to ensure the adequate perfusion of all the vital organs.
Hepatic Coagulopathy
Severe hepatic disease is associated with abnormalities of the coagulation system. The cause is multifactorial and may include the decreased synthesis of procoagulant proteins, impaired clearance of activated coagulation factors, nutritional deficiency (eg, vitamin K, folate), the synthesis of functionally abnormal fibrinogen, splenomegaly secondary to portal hypertension (sequestrational thrombocytopenia), qualitative platelet defects, and bone marrow suppression of thrombopoiesis (eg, by alcohol, hepatitis virus infection). Because of the potential complexity of the coagulopathy, it may be necessary to perform additional laboratory tests such as clotting factor and fibrinogen assays to completely delineate the nature of the problem. Clotting factor deficiencies can be treated with vitamin K supplementation fresh frozen plasma transfusion, or both. Platelet transfusion maybe necessary in the case of thrombocytopenia. Other therapies such as recombinant factor VIIa have also been used to correct bleeding associated with liver failure.
Since the vitamin K–dependent clotting factors are more susceptible to hepatocellular disease, the prothrombin time (PT) and international normalized ratio (INR) are often used as markers of coagulation system integrity. However, the predictive value of PT/INR on hemorrhage during bedside procedures such as lumbar puncture or central line placement has been shown to be poor. As such, it is important to carefully weigh the risks and benefits of a neuraxial anesthetic technique in a patient with suspected hepatic-induced coagulopathy.
Although an INR of less than 1.5 “should be associated with normal hemostasis” according to the American Society of Regional Anesthesia and Pain Medicine (ASRA) consensus guidelines on anticoagulation, this statement applies primarily to warfarin-induced anticoagulation and may not be a reliable indicator of the likelihood of problematic bleeding in liver failure. Epidural analgesia is frequently used during and following major liver resection, although there are some safety concerns as postoperative derangement of coagulation parameters is common; however, there are no reports of epidural hematoma in this setting. The risks associated with performing peripheral nerve blocks in patients with abnormal coagulation parameters are less clear. Obviously, the risk of bleeding is increased with techniques in which the needle is placed in the vicinity of a major blood vessel. Careful consideration of risks and benefits should be performed when considering lumbar plexus block in coagulopathic patients, as a retroperitoneal hemorrhage in this space may be extensive and not obvious until the patient is in shock. Likewise, care should be taken when performing blocks in the vicinity of noncompressible blood vessels (eg, the subclavian artery in the case of infraclavicular block) in patients who have a coagulation abnormality. The risks of regional anesthesia in the setting of a disorder are elaborated on in “Regional Anesthesia in the Critically Ill“.
NYSORA Tips
- Deep blocks, such as anterior sciatic or lumbar plexus blocks, should be practiced with special care in patients with coagulopathy.
- Similarly, blocks in the vicinity of noncompressible blood vessels, such as the artery in the fossa, should be carefully considered.
DIABETES MELLITUS
Diabetes is a multisystem disease characterized by carbohydrate intolerance and insulin dysregulation that has many implications for the regional anesthesiologist. Besides the usual anesthetic concerns, such as the presence of coronary artery, cerebrovascular, and renal disease, diabetics have a high incidence of preexisting peripheral neuropathy, which has implications for block performance and success and poses a risk for neurologic complications. Other considerations are the effect of regional anesthesia on glucose homeostasis and the increased risk of infection in diabetic patients.
Peripheral Neuropathy in Diabetics
Diabetic neuropathy is one of the most common neurologic diseases, affecting up to 100% of diabetic patients with long-standing disease. Patients can be asymptomatic, but in affected patients, symptoms are typically described as paresthesias, sensory loss, or neuropathic pain. The mechanism of diabetic neuropathy is thought to be related to either a direct metabolic and osmotic effect of chronic hyperglycemia on neurons or a microvascular insult leading to nerve ischemia.
Performing nerve blocks in patients with peripheral neuropathy is controversial. Kalichman and Calcutt studied sciatic nerve histology in rats following block with lidocaine and found significantly more nerve edema in the nerves of the rats with diabetes versus healthy controls. The reason for the edema is probably multifactorial and may include the presence of an altered blood-nerve barrier or decreased uptake of local anesthetic, leading to a longer duration of nerve bathing. An increase in endoneural fluid pressure due to edema may constrict small transperineural vessels, precipitating ischemia in an already compromised nerve. This may translate to an increased incidence of postoperative paresthesias following nerve blocks, including neuraxial blocks, in diabetics. Al-Nasser reported a case of prolonged (> 8 weeks) bilateral lower limb paresthesias and pain following lumbar epidural analgesia with 0.2% ropivacaine in a diabetic patient undergoing radical prostatectomy. Postoperative electromyographic studies showed widespread sensory neuropathy of both upper and lower limbs, indicating that the patient, although asymptomatic, had preexisting neuropathy that may have predisposed him to this rare complication. Studies have demonstrated a prolonged duration of sensory and motor block following sciatic nerve block in diabetics when compared to nondiabetics and that the duration of block increases as glycemic control worsens (as measured by glycosylated hemoglobin levels). A study in diabetic rats showed a similar prolongation of local anesthetic effect which was reversed by 2 weeks of insulin treatment but unaffected by 6 hours of insulin, suggesting that the increased sensitivity to local anesthetics is mediated by chronic changes in the nervous system as opposed to the current blood glucose level. It is unclear whether this increased sensitivity to local anesthetics represents an increased risk of neurological complications. The actual prevalence of neurologic complications in diabetics receiving nerve blocks is unknown but is probably quite low. Diabetes is a common disease, and reports of neurologic complications in the literature are sparse, suggesting that in the vast majority of cases, recovery from peripheral nerve blocks is uneventful.
Patients with diabetes should also be considered at increased risk for infectious complications of regional anesthesia due to the immune suppression that occurs as a result of the disease. Diabetes has been implicated as a risk factor for infection following both peripheral and neuraxial block. Although it is unclear to what extent diabetes truly increases the risk of infection, it seems wise to be extra vigilant with infection control precautions in these patients.
The effect of diabetic neuropathy on electrolocation of nerves while using a nerve stimulator is another matter of controversy. Patients with long-standing diabetes may require somewhat higher current intensity in order to produce a motor response. While nerve conduction studies in diabetics with neuropathy consistently show a reduction in conduction velocity and amplitude for both motor and sensory nerves, this does not tend to be the case in actual clinical practice, as most patients with diabetes have similar current intensity thresholds as non-diabetic patients without neuropathy.
NYSORA Tips
- Patients with diabetes are prone to a metabolic neuropathy that impairs nerve conduction.
- A stimulating current of greater intensity is only occasionally needed to obtain visible muscle twitches when using a nerve stimulator to electrolocate nerves.
Effect of Regional Anesthesia on Glucose Homeostasis
It is well known that surgery performed in combination with general anesthesia provokes a counterregulatory response that significantly increases plasma levels of glucose, as well as levels of cortisol and catecholamines. This so-called stress response has long been considered a homeostatic defense mechanism that is important in an organism’s adaptation to harmful stimuli, providing substrates for energy in times of need. However, prolonged periods of hyperglycemia may have deleterious effects on patients, with evidence supporting an increase in mortality rates, hospital length of stay, and incidence of nosocomial infection. Hyperglycemia may be particularly hazardous in patients who have incurred trauma.
Regional anesthesia has been shown to ameliorate the hyperglycemic response to surgery and therefore may play a role in this protective phenomenon. An intraoperative glucose tolerance test resulted in markedly elevated plasma glucose levels in patients receiving general versus epidural anesthesia for such procedures as inguinal herniorrhaphy and hysterectomy. Likewise, abdominal hysterectomy performed under spinal anesthesia is associated with lower intra- and postoperative glucose levels compared with neuroleptanesthesia. Retrobulbar block reduces the hyperglycemic stress response to both cataract and scleral buckle surgery.
Glucose homeostasis is complex, and several factors likely contribute to the salutary action of regional anesthesia on glycemic control. These may include the inhibition of hepatic gluconeogenesis as well as the inhibition of catecholamine and cortisol responses to surgery. In addition, the “absence of general anesthesia” may be a causative factor in glycemic control, as volatile agents such as halothane and enflurane have been shown to impair glucose tolerance in dogs. It seems clear from the available data that to improve outcomes from major surgery, anesthesiologists must prevent as much nociceptive input from reaching the central nervous and neuroendocrine systems as possible. The use of regional anesthesia can easily facilitate this goal and may be especially pertinent for “brittle” diabetics in whom tight glycemic control is difficult at the best of times.
THYROID NEUROPATHY
Diabetes and uremia are the most common metabolic neuropathies; however, several other less common neuropathies also have implications for the regional anesthesiologist. These include those neuropathies that result from the use of certain medications or exposure to toxins and those related to connective tissue, autoimmune, and vascular diseases. One of the most prevalent causes of metabolic neuropathy is that associated with overt hypothyroidism. Thyroid neuropathy is a largely sensory phenomenon that is poorly understood but present in approximately 40% of patients diagnosed with hypothyroidism. It is most obvious in frank myxedema, but nerve conduction studies have shown evidence of velocity impairment in subclinical hypothyroidism. Thyroid neuropathy is most likely to present as peripheral nerve entrapment, particularly of the median nerve, and these patients are frequently referred for carpal tunnel decompression. Entrapment of the eighth cranial nerve leading to deafness is also common. Patients may complain of dysesthesias in a glove-and-stocking pattern, as well as lancinating pains suggestive of nerve root compression. “Hung” deep tendon reflexes (brisk reflex response with a delayed return to normal tone) are a hallmark of hypothyroidism and probably relate to both neuropathy and myopathy. Pathologically, affected nerves exhibit mucinous deposition and, in advanced cases, segmental demyelination with loss of large myelinated nerve fibers.
Few data exist on the effect preexisting thyroid neuropathy may have on the management of regional anesthesia in this population. A potential consequence of performing regional anesthesia in patients with nerve entrapment is what has been termed the “double-crush syndrome.” This refers to the enhanced susceptibility of nerves to injury or impairment at one anatomic location when already compressed or otherwise injured at another, separate location. A classic example is the patient with symptoms of carpal tunnel syndrome after seemingly minor trauma or injury to the median nerve, who is later found to have compression of the C6 nerve root. Although originally described in terms of mechanical injury, it has been recognized that metabolic and pharmacologic factors can contribute to the double-crush syndrome, including hypothyroidism. Thus, it may be that patients with thyroid neuropathy are at increased risk for neurologic injury when receiving regional anesthesia blocks, as minor needle trauma to a susceptible nerve may produce functional neurologic deficits. Although this remains speculative at present, this possibility reinforces the need for a detailed history and documentation of preexisting neurologic deficit in patients with hypothyroidism and the careful consideration of techniques in these patients. Finally, if suspected, thyroid neuropathy has been shown to be correctable in many cases by prompt treatment with thyroid replacement therapy, which may this complication.
OBESITY
Obesity is an increasingly prevalent problem, with worldwide obesity rates have doubled since 1980. Over the last 20 years, there has been a dramatic rise in obesity in the U.S., with 35% of adults and 17% of children and adolescents meeting the criteria for obesity in 2012. In addition to the usual anesthetic considerations for morbidly obese patients, such as the presence of various cardiopulmonary, gastrointestinal, and endocrine comorbidities, the abundance of extra tissue can present a challenge to regional anesthesiologists. Obesity has been shown to impair the ability of anesthesiologists to correctly identify lumbar spinal interspaces. Outcomes are similarly affected in overweight patients. In a study of over 9000 mixed blocks at a single institution, patients with a body mass index (BMI) greater than 30 kg/m2 were 1.62 times more likely to experience a failed regional block than were those with a BMI less than 25 kg/m2. Not surprisingly, the investigators cited difficulty in landmark identification, patient positioning, and insufficient length of needle used as the main impediments to successful block placement. These findings are supported by a study of axillary blocks using nerve stimulator guidance, where obesity was associated with longer block performance time, decreased success rate, increased complication rate, and decreased patient satisfaction. Despite these relative difficulties, block success rates in obese patients were high, and rates of serious complications were low. Regional anesthesia remains an attractive option for obese patients because it may reduce the incidence of cardiopulmonary and airway complications compared with those experienced during general anesthesia.
NYSORA Tips
- Obese patients are more likely to experience a failed regional block than patients with a BMI within the normal range.
- Reasons for this include difficult surface or sonographic landmarks, difficulty in patient positioning.
Obese patients seem to benefit from image-guided regional anesthetic blocks. Fluoroscopy has been used in the placement of axillary brachial plexus catheters, in the performance of sciatic nerve blocks, and as an aid in facilitating spinal anesthesia in morbidly obese patients. However, its use is limited by the need to relate neural anatomy to structures that appear radiodense, such as bones, needles, or contrast-injected vessels.
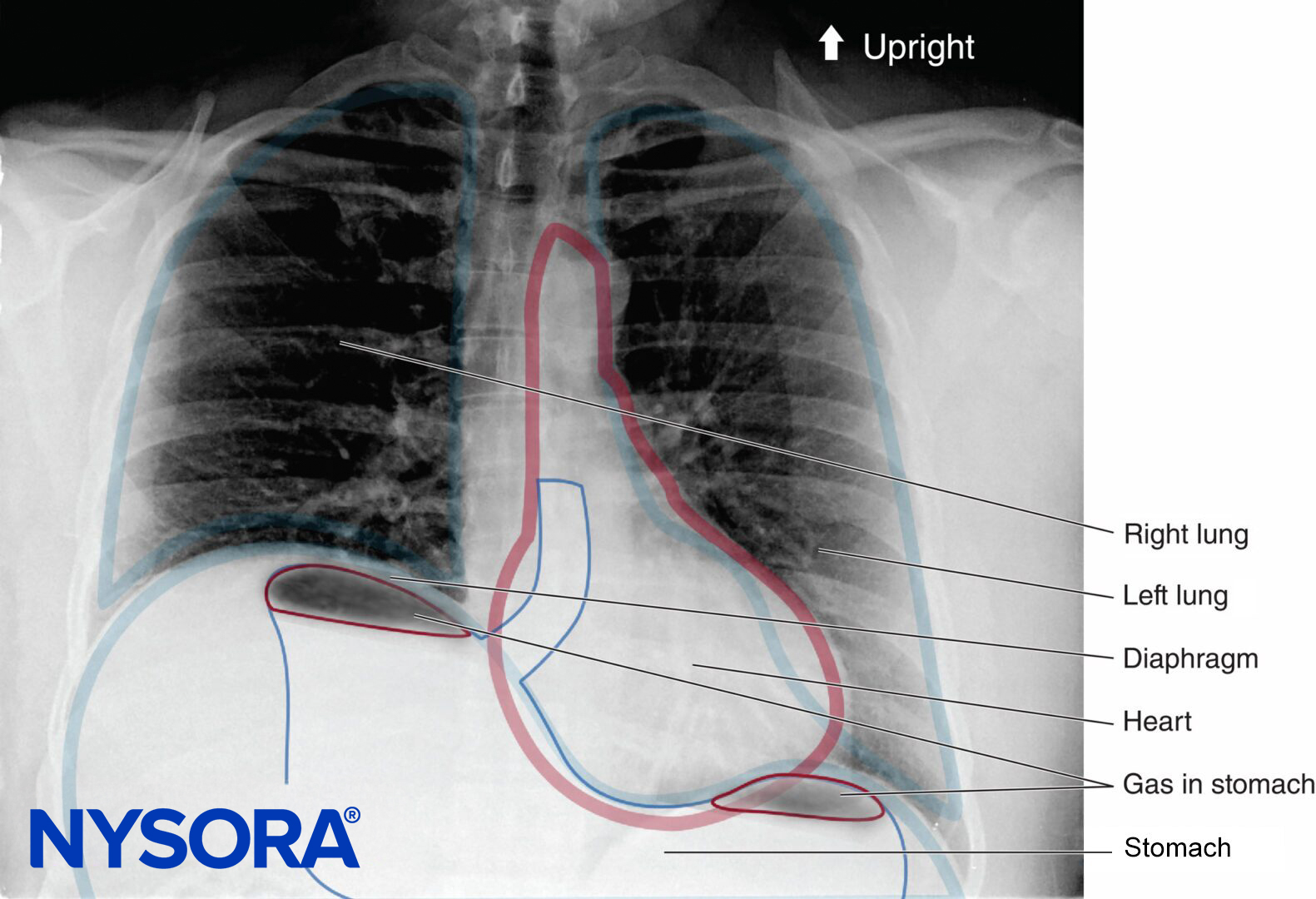
Ultrasound may be especially useful in obese patients with obscured surface landmarks, although excess adipose tissue can make ultrasound examination itself more difficult due to attenuation of the ultrasound beam. This difficulty can be partly overcome by decreasing the frequency of the transducer to increase penetration depth, although image resolution will be reduced (Figure 2). When median and sciatic nerves were scanned in normal-weight and obese volunteers, Marhofer et al. concluded that visualization of superficial peripheral nerves is independent of BMI, whereas deeper nerves are more difficult to visualize in obese subjects. Studies conducted in obese parturients and in nonobstetric patients with difficult surface anatomic landmarks have verified the utility of ultrasound in identifying the epidural space and other spinal structures prior to the performance of a neuraxial block. To date, few studies have compared ultrasound-guided peripheral nerve blocks with landmark or nerve stimulator–guided techniques in the obese population; however, ultrasound seems to be a useful modality for this potentially challenging group of patients.
 patient and a slim (2) patient. Note the increased depth required to image the artery (A) and nerve (dotted outline) in the obese example, as well as the overall poor resolution quality due to the excess adipose tissue. In contrast, the nerve, artery, muscles, and fascial planes in the slim patient are crisp and well defined.")
FIGURE 2. Ultrasound scans of the femoral regions in an obese (1) patient and a slim (2) patient. Note the increased depth required to image the artery (A) and nerve (dotted outline) in the obese example, as well as the overall poor resolution quality due to the excess adipose tissue. In contrast, the nerve, artery, muscles, and fascial planes in the slim patient are crisp and well defined.
Obesity may have an effect on the dosing of spinal medications, although the issue is somewhat controversial. A common notion is that increased abdominal mass leads to compression of intrathecal volume by engorgement of epidural plexuses, leading to an increased, and potentially dangerous, block height during spinal anesthesia. This is supported by data correlating block height with patient weight during standardized spinal anesthesia for cystoscopy. Indeed, some authors have advocated the consideration of “low-dose” spinal anesthesia in the morbidly obese, due to wide variations in their dosing requirements. In one extremely overweight parturient (BMI = 66 kg/m2), cesarean section was completed successfully with a 5-mg spinal dose of bupivacaine as the sole anesthetic agent. However, patient weight does not necessarily correlate with the degree of compression of the thecal sac, and many investigators have argued that weight alone is not a reliable predictor of block height during spinal anesthesia. A dose-finding study of hyperbaric bupivacaine in patients undergoing knee replacement found no difference in the dose required to achieve a block to T12 between obese and nonobese patients but did find a slightly longer duration of block and reduced incidence of tourniquet pain in the obese group. However, no patients in the obese group had a BMI over 40, so these findings may not be reflective of the morbidly obese population. It is probably reasonable to approach the spinal dosing of morbidly obese patients with a degree of caution, and when practical, to incrementally adjust the anesthetic dose.
Clinical updates
Polderman et al. (BJA Education, 2024) provide an updated framework for perioperative diabetes management, focusing on modern therapies and devices. Key updates include perioperative withholding of SGLT2 inhibitors due to the risk of euglycaemic ketoacidosis, nuanced guidance on GLP-1 receptor agonists that balances aspiration risk against metabolic benefit, and reinforcement that basal–bolus insulin regimens are superior to sliding-scale insulin postoperatively, with CGMs and insulin pumps used only with caution and with confirmatory capillary glucose checks.
Chowdhury & McLure (BJA Education, 2022) review perioperative implications of chronic kidney disease, highlighting that CKD confers multisystem risk dominated by cardiovascular disease, fluid and electrolyte instability, and altered drug pharmacokinetics. They emphasize recent guidance on estimating renal function using the CKD-EPI equations without ethnicity correction, careful avoidance of nephrotoxins, and preferential use of short-acting, non–renally cleared anaesthetic drugs (e.g., atracurium), with vigilant fluid and haemodynamic management to prevent perioperative AKI.