

A breakthrough randomized controlled trial by Trocheris-Fumery et al. reveals that the early administration of norepinephrine during anesthesia induction significantly reduces postoperative complications in high-risk patients undergoing major abdominal surgery.
Background
Intraoperative hypotension, a common drop in blood pressure following the induction of anesthesia, has long been associated with adverse outcomes, including:
- Myocardial injury
- Acute kidney injury (AKI)
- Increased mortality risk
Despite this, standard vasopressor regimens vary, and evidence comparing strategies for preventing such hypotension is limited.
Study overview
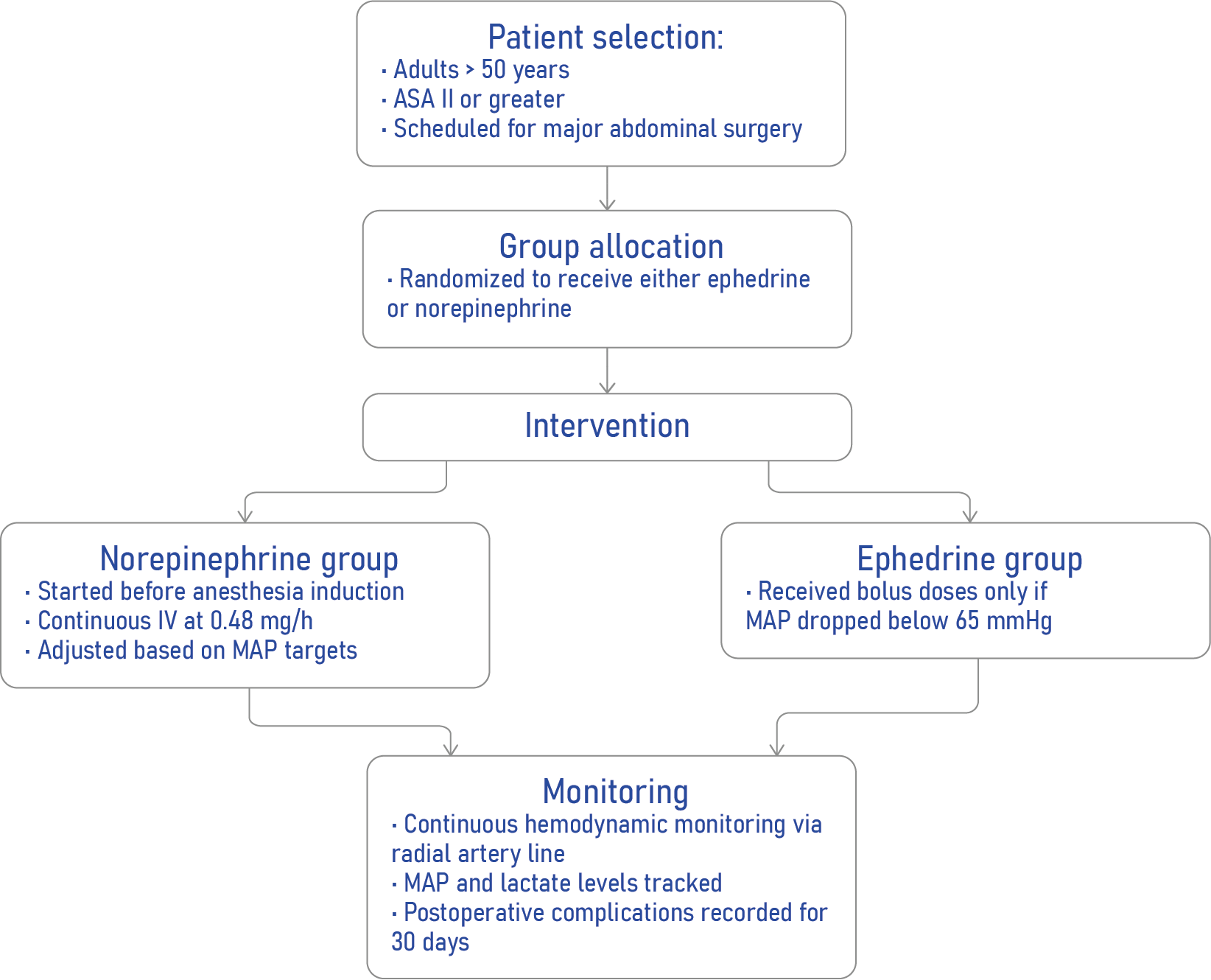
A research team at Amiens Hospital University in France conducted the EPON trial (Early Use of Norepinephrine), a single-center, randomized controlled study, to evaluate whether prophylactic norepinephrine infusion could better prevent postinduction hypotension and its associated complications compared to standard treatment with reactive ephedrine boluses.
Key study details:
- Design: Prospective, randomized, open-label, single-center
- Patients: 500 adults aged >50 undergoing major abdominal surgery
- Groups:
- Norepinephrine group: Prophylactic continuous infusion (0.48 mg/h)
- Ephedrine group: Reactive boluses (3 mg each, max 30 mg)
- Norepinephrine group: Prophylactic continuous infusion (0.48 mg/h)
How the intervention works
Core findings
Reduction in complications
- Primary endpoint: Medico-surgical complications within 30 days (Clavien–Dindo score ≥1)
- Ephedrine group: 58%
- Norepinephrine group: 44%
- Relative risk (RR): 0.58 [0.40–0.83]; P = 0.004
- Ephedrine group: 58%
Pulmonary benefits
- Postoperative pulmonary complications (PPCs) at 48 hours:
- Ephedrine: 31%
- Norepinephrine: 17%
- Ephedrine: 31%
Hemodynamic stability
- Hypotensive episodes occurred in:
- 74% of ephedrine group
- Only 15% of the norepinephrine group
- Norepinephrine also resulted in:
- Higher mean arterial pressure (MAP) post-induction
- Lower intraoperative lactate levels (suggesting better organ perfusion)
- Higher mean arterial pressure (MAP) post-induction
How norepinephrine works
Norepinephrine is a potent α1- and β1-adrenergic agonist, leading to:
- Vasoconstriction (↑ blood pressure)
- Improved cardiac output
- Stable hemodynamics during anesthesia induction
Unlike ephedrine, it avoids tachyphylaxis (diminished effect with repeated use) and is increasingly considered for first-line vasopressor use in anesthesia.
Subgroup insights
Norepinephrine was especially effective in reducing complications among:
- ASA III patients
- Men
- Patients without CKD
- Patients undergoing digestive surgery
Conclusion
Early, titrated norepinephrine infusion significantly reduces both hypotension and postoperative complications in high-risk patients undergoing major abdominal surgery. This proactive approach challenges conventional vasopressor strategies and may redefine intraoperative care in anesthesia.
Reference: Trocheris-Fumery O et al. Early Use of Norepinephrine in High-risk Patients Undergoing Major Abdominal Surgery: A Randomized Controlled Trial. Anesthesiology. 2025;143:1160-1170.
Download the AA App now to put trusted anesthesia guidance in your pocket.