


Laparoscopic colorectal surgery (LCS) has become standard practice for many colorectal procedures, offering smaller incisions, faster mobilization, and shorter hospital stays than open surgery. Yet even with minimally invasive techniques, patients frequently experience substantial postoperative pain—driven by trocar sites, deep myofascial trauma, pneumoperitoneum, and visceral manipulation. This pain can delay mobilization, increase opioid requirements, and undermine enhanced recovery after surgery (ERAS) pathways.
Systemic multimodal analgesia alone often falls short, and neuraxial techniques are not always desirable in LCS due to hypotension, urinary retention, and resource implications. Fascial plane blocks are increasingly used as opioid-sparing adjuncts, but most (like standard TAP blocks) primarily address somatic pain and offer limited visceral coverage.
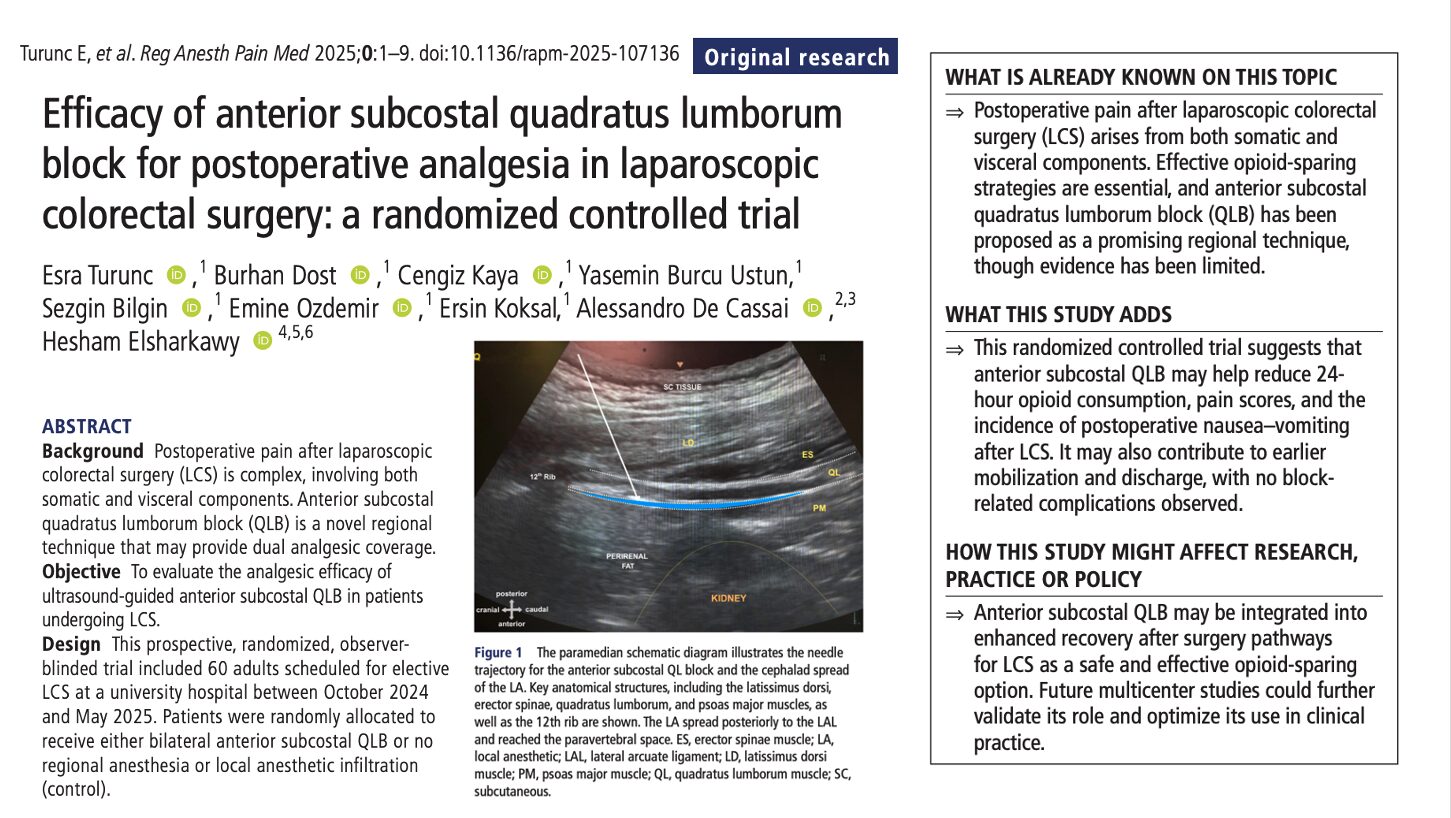
The anterior subcostal quadratus lumborum block (QLB) is designed to reach higher thoracic dermatomes and potentially the thoracic paravertebral space, targeting both somatic and visceral nociceptive pathways. Anatomical and early clinical data suggest coverage from about T7 to L1 or higher, which aligns well with typical LCS incision patterns and intra-abdominal pain sources.
However, robust data for anterior subcostal QLB specifically in laparoscopic colorectal surgery have been limited. This randomized controlled trial set out to test whether adding an ultrasound-guided anterior subcostal QLB to standardized multimodal care could meaningfully reduce opioid requirements and improve early recovery after LCS.
Study objective and methods
The primary objective was to compare 24-hour postoperative opioid consumption (intravenous morphine milligram equivalents, MME) between patients receiving bilateral anterior subcostal QLB and those receiving no regional block for LCS.
- Design: Single-center, prospective, randomized, controlled, observer-blinded trial.
- Setting: University hospital in Türkiye.
- Population: 60 adults (ASA I–III) scheduled for elective laparoscopic colorectal surgery; 55 analyzed (QLB n = 27, control n = 28) after excluding conversions to open surgery.
- Intervention group: Bilateral anterior subcostal QLB performed ~ 30 minutes pre-op with 20 mL 0.25% bupivacaine with epinephrine (1:400,000) per side, using an ultrasound-guided approach between quadratus lumborum and psoas major near the 12th rib.
- Control group: No block and no local anesthetic infiltration.
- All patients received standardized general anesthesia, multimodal analgesia, and PCA morphine.
- Secondary outcomes included 12-hour opioid use, pain scores at rest and with movement, time to first PCA demand, rescue analgesia and antiemetic use, block-related complications, dermatomal spread, time to mobilization, and hospital length of stay.
Key findings
-
Opioid consumption and analgesia
Anterior subcostal QLB produced a clear opioid-sparing effect. At 12 hours, median IV MME use was 8 mg (IQR 2–15) with QLB versus 15.1 mg (12–18.1) in controls. By 24 hours, the QLB group had used 15 mg (6.5–22) versus 24.3 mg (20.3–30.3) in the control group. Pain scores at rest and with activity were significantly lower in the QLB group at every measured time point from PACU through 24 hours, indicating that reduced opioid use reflected genuine analgesic benefit rather than underuse of PCA.
-
PCA behavior, rescue therapy, and PONV
The QLB group waited longer before their first PCA demand (median 45 vs 20 minutes), and very few required additional rescue analgesia in the first 24 hours (7.4% vs 92.8% in controls). Antiemetic use was also markedly lower with QLB (18.5% vs 71.4%), consistent with lower opioid exposure and more stable postoperative comfort, though PONV is multifactorial.
-
Dermatomal coverage and safety
Sensory testing at 30 minutes showed reproducible spread across T7–L1 in all QLB patients, with partial extension to T6 in 63% and to T4–T5 in 15%. This distribution matches the area involved in laparoscopic colorectal surgery incisions and visceral discomfort. No block-related complications were observed: there were no cases of local anesthetic systemic toxicity, retroperitoneal hematoma, or visceral injury in this series.
-
Early recovery signals
Patients who received QLB mobilized earlier and left hospital slightly sooner. Median time to first mobilization was 12 hours (IQR 10–18) versus 17 hours (12–20) in controls, and median length of stay was 5 days (5–6) versus 6 days (5–7). These differences are modest and influenced by many non-analgesic factors, but they are directionally consistent with better pain control and fewer opioid-related side effects.
Conclusion
In patients undergoing laparoscopic colorectal surgery, a bilateral anterior subcostal QLB added to standardized multimodal analgesia reduced 12- and 24-hour opioid consumption, lowered pain scores at rest and with movement, reduced rescue analgesia and PONV, and modestly accelerated mobilization and discharge. No block-related complications were observed. While the absolute opioid reduction is moderate, the overall pattern supports anterior subcostal QLB as a useful ERAS-compatible adjunct for LCS rather than a standalone solution.
Future research
- Multicenter trials to confirm efficacy and safety across varied teams and ERAS pathways.
- Comparisons versus TAP, ESP, and epidural strategies for LCS.
- Evaluation of continuous or catheter-based QLB vs single-shot techniques.
- Imaging-based studies of in vivo injectate spread during pneumoperitoneum.
- Determination of procedure-specific MCID thresholds for opioid reduction and pain scores in LCS.
Clinical implications
For teams managing laparoscopic colorectal surgery, anterior subcostal QLB offers a practical way to enhance multimodal analgesia without adding neuraxial risk. It provides broad thoracolumbar coverage, lowers opioid needs, improves comfort, and reduces PONV in the first 24 hours—key targets in ERAS programs. That said, the effect size is moderate and should be seen as an incremental gain rather than a complete solution. Success hinges on proper sonoanatomy, technique, and integration with robust systemic multimodal regimens.
Clinical pearls
- Anterior subcostal QLB reduced 24 h IV opioid use by ~ 9 mg MME.
- Pain scores (rest and movement) were significantly lower at all time points.
- Rescue opioids and antiemetics were needed in far fewer QLB patients.
- Dermatomal coverage was typically T7–L1, sometimes extending to T5–T6.
- No block-related complications were reported in this single-center trial.
Practical tip: Consider a bilateral anterior subcostal QLB as an ERAS-friendly add-on for LCS when expertise and ultrasound imaging quality are available.
For more detailed information, refer to the full article in RAPM.
Turunc E. et al. Efficacy of anterior subcostal quadratus lumborum block for postoperative analgesia in laparoscopic colorectal surgery: a randomized controlled trial. Reg Anesth Pain Med. Published online October 28, 2025.
Refine your QL block technique—dosing, spread patterns, and expert insights in the NYSORA Nerve Blocks App.