Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe diabetes insipidus
- Recognize the symptoms and signs of diabetes insipidus
- Anesthetic management of a patient with diabetes insipidus
Definition and mechanisms
- Diabetes insipidus (DI) is a disorder of urinary concentration caused by a temporary or chronic deficiency of or insensitivity to antidiuretic hormone (ADH) or vasopressin
- The condition renders the kidneys unable to effectively autoregulate water balance, resulting in polyuria, polydipsia, and electrolyte abnormalities (e.g., hypernatremia, hypokalemia)
Classification
- Central DI or ADH deficiency: Reduced ADP secretion due to damage to the pituitary gland or hypothalamus or genetics
- Nephrogenic DI or ADH resistance: Normal ADP secretion, but the kidneys are unable to properly respond to ADH due to an inherited genetic disorder or chronic kidney disorder
- Gestational DI: A very rare condition that occurs during pregnancy when an enzyme made by the placenta destroys ADH
- Primary polydipsia (dipsogenic DI): Damage to the hypothalamic thirst center causes excessive fluid intake leading to polyuria
Signs and symptoms
| Adults | Children | Infants |
|---|---|---|
| Polyuria Polydipsia Nocturia Craving for ice water | Anorexia Growth defects Enuresis Sleep disturbance Fatigue | Irritability Chronic dehydration Growth retardation Neurologic disturbance Hyperthermia |
Clinical findings
- If the thirst mechanism is intact: Hydronephrosis and distended bladder due to excessive urinary volume
- If there is no access to free water or damage to the hypothalamic thirst center: Hypernatremia, dehydration, hypertonic encephalopathy, obtundation, coma, seizure, subarachnoid hemorrhage, and intracerebral hemorrhage
Complications
Dehydration, which may cause:
- Dry mouth
- Changes in skin elasticity
- Thirst
- Fatigue
Electrolyte imbalance, resulting in:
- Weakness
- Nausea
- Vomiting
- Loss of appetite
- Muscle cramps
- Confusion
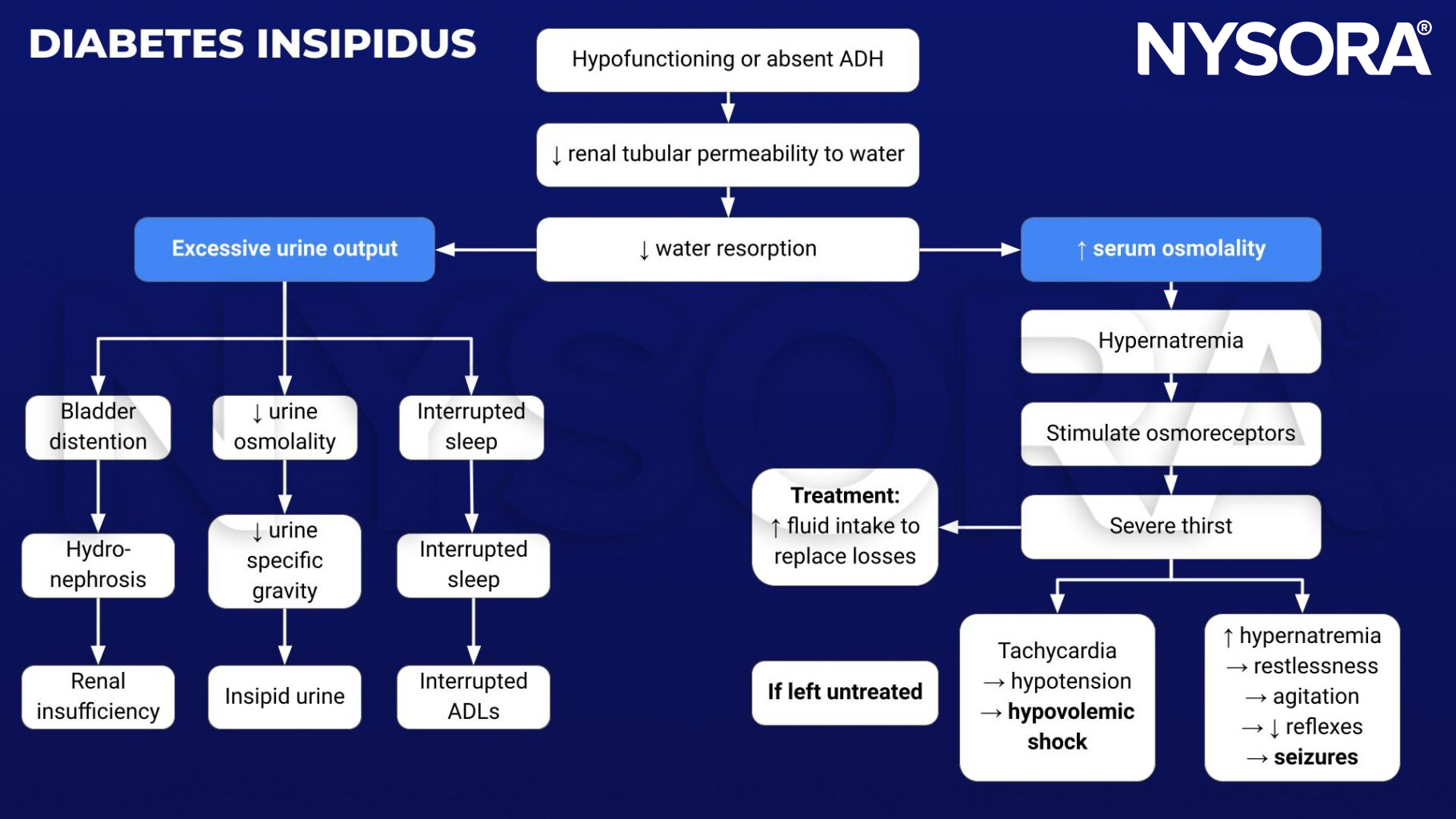
Pathophysiology
Treatment
There is no cure → treatments aim to relieve thirst, decrease urine output, and prevent dehydration
- Central and gestational DI: Desmopressin (DDAVP)
- Nephrogenic DI: Treat the underlying cause or use a thiazide, aspirin, or ibuprofen
- Primary polydipsia: Decrease fluid intake
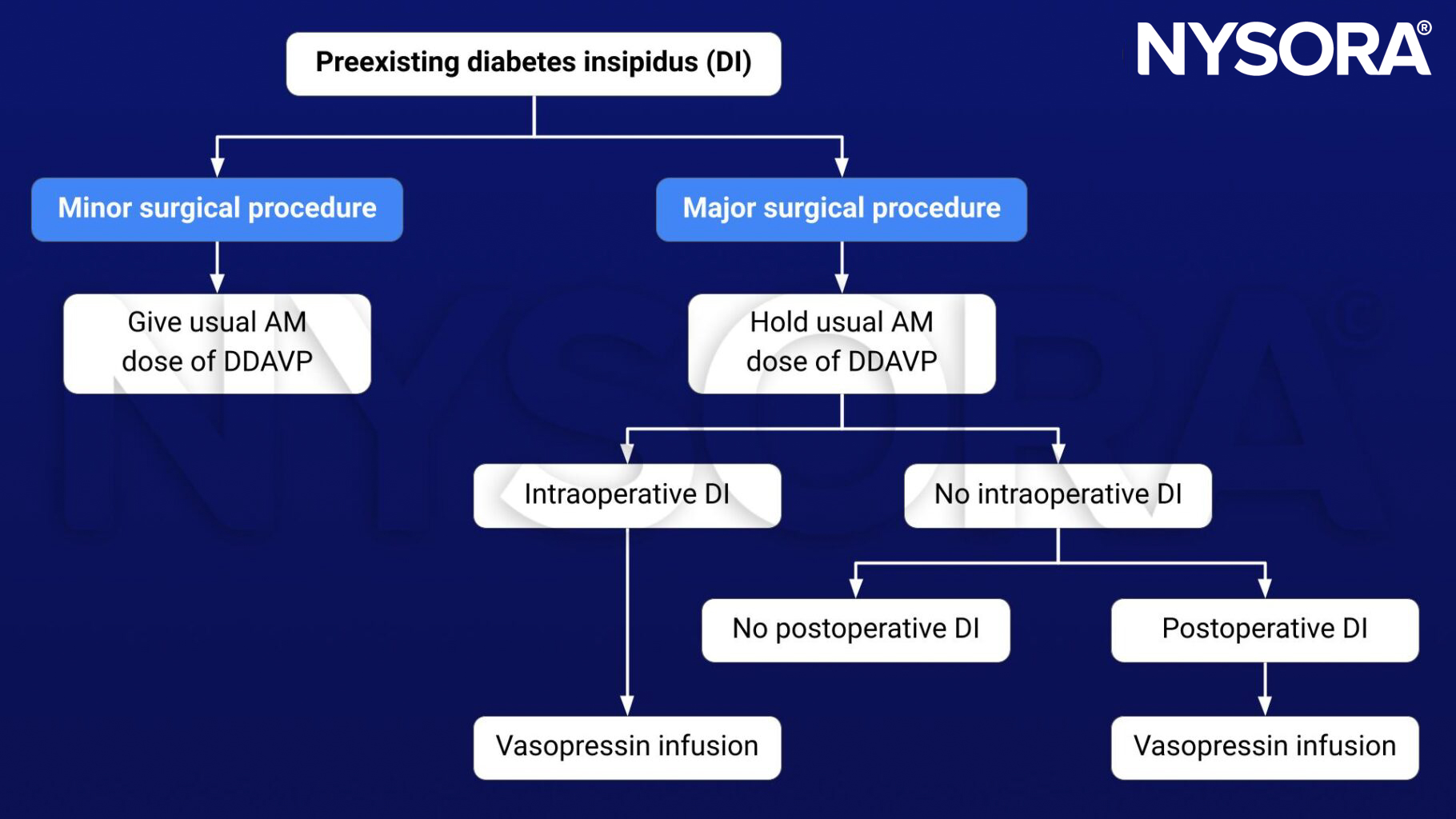
Management
- Hypernatremia: ↑ MAC requirements
- Treat hypernatremia by estimating water deficit and replacing it with free water:
- Water deficit = total body water x (Serum Na [ ]/140-1)
- Volume depletion: Resuscitate with normal saline initially
- Central DI: DDAVP 1-2 mcg i.v. BID
- Nephrogenic DI: Hydrochlorothiazide/amiloride
Keep in mind
- Avoid rapid overcorrection if chronic hypernatremia (goal = <10 mEq/day)
- Be careful of cerebral edema, water intoxication, and volume overload
Suggested reading
- Mutter CM, Smith T, Menze O, Zakharia M, Nguyen H. Diabetes Insipidus: Pathogenesis, Diagnosis, and Clinical Management. Cureus. 2021;13(2):e13523.
- Dharshan AC, Kohli-Seth R. Chapter 117. Diabetes Insipidus. In: Atchabahian A, Gupta R. eds. The Anesthesia Guide. McGraw Hill; 2013. Accessed January 17, 2023.