Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About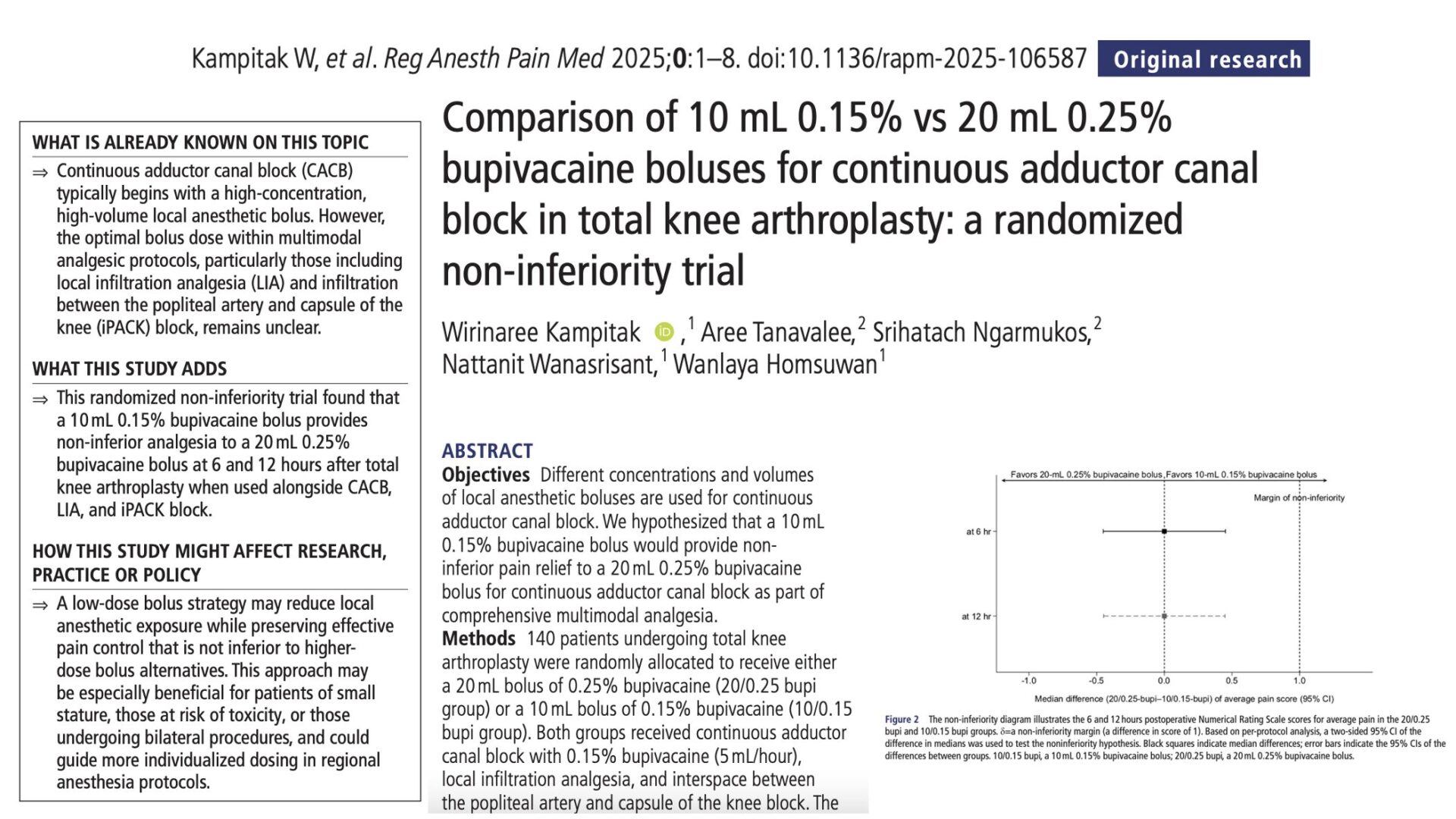





Total knee arthroplasty (TKA) is one of the most commonly performed orthopedic procedures worldwide, with increasing emphasis on enhanced recovery after surgery (ERAS) protocols. Effective postoperative analgesia is crucial to support early mobilization, reduce opioid consumption, and improve patient satisfaction.
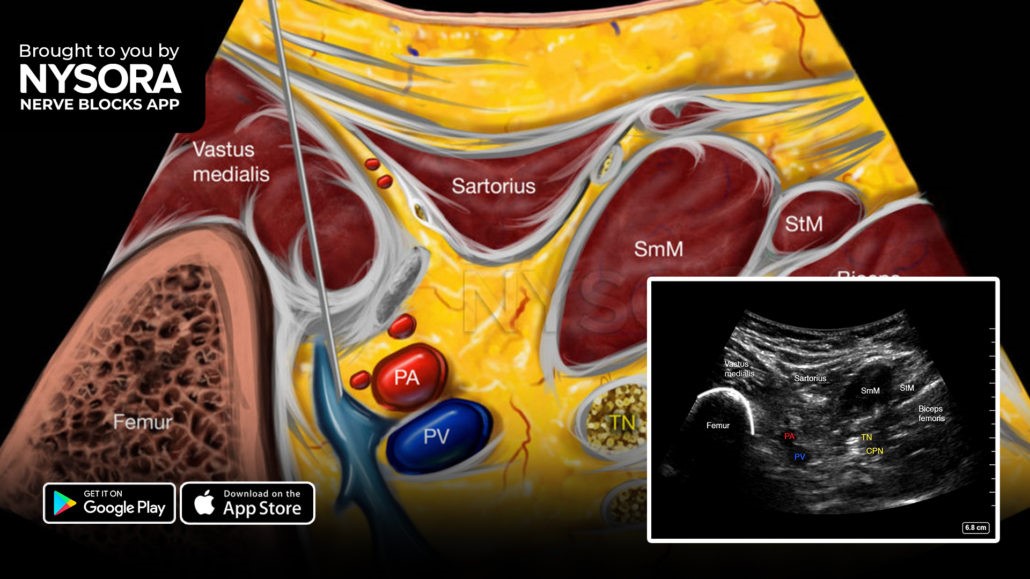
The adductor canal block (ACB) has become a cornerstone of regional anesthesia in TKA due to its motor-sparing profile and targeted analgesia of the anteromedial knee. In continuous ACB, boluses of local anesthetic are often administered via catheter to extend pain relief. However, there is little consensus on the optimal concentration and volume of local anesthetic for these boluses.
This randomized non-inferiority trial, led by Kampitak et al., aimed to determine whether a low-volume, low-concentration bupivacaine bolus could provide pain relief comparable to a higher-volume, higher-concentration alternative. The results carry important implications for minimizing local anesthetic use while maintaining analgesic efficacy in TKA patients.
Study objective and methods
The study’s primary objective was to assess whether a 10 mL bolus of 0.15% bupivacaine is non-inferior to a 20 mL bolus of 0.25% bupivacaine in managing postoperative pain via continuous adductor canal block in patients undergoing total knee arthroplasty.
This was a prospective, randomized, non-inferiority trial conducted at King Chulalongkorn Memorial Hospital in Bangkok, Thailand. The study enrolled 140 adult patients scheduled for primary unilateral TKA under spinal anesthesia, all of whom received multimodal analgesia including:
- Continuous adductor canal block with 0.15% bupivacaine at 5 mL/hour.
- Intraoperative local infiltration analgesia.
- A single-shot iPACK (interspace between the popliteal artery and capsule of the knee) block.
Participants were randomized into two groups:
- 20/0.25 group: Received a 20 mL bolus of 0.25% bupivacaine.
- 10/0.15 group: Received a 10 mL bolus of 0.15% bupivacaine.
The bolus was administered at the end of surgery through the catheter. Pain scores were assessed using an 11-point numeric rating scale (NRS). The primary outcome was average pain score at 6 and 12 hours postoperatively. A non-inferiority margin of 1 point on the NRS was predefined. Secondary outcomes included pain at rest and during movement, total morphine consumption, and time to first rescue analgesia.
Key findings
-
Pain scores at rest and during movement
Pain relief was comparable between the two dosing regimens. At 6 hours postoperatively, median pain scores were 0 in both groups, though the 10/0.15 group had a slightly broader interquartile range (0–2 vs. 0–1). At 12 hours, both groups reported a median score of 2, again with similar interquartile ranges. Importantly, the calculated median treatment difference between groups was zero, and the 95% confidence interval (−0.45 to 0.45) fell within the pre-specified non-inferiority margin of 1. This confirmed statistical non-inferiority of the lower-dose bolus.
-
Opioid consumption and rescue analgesia
Cumulative morphine use within the first 12 hours was similar in both groups. The time to first rescue analgesic did not differ significantly, suggesting that patients receiving the lower-dose bolus were not more likely to experience breakthrough pain or require additional medications.
-
Overall analgesic equivalence
These results collectively demonstrate that the lower-volume, lower-concentration bolus (10 mL of 0.15% bupivacaine) provided pain control equivalent to that of the traditional 20 mL of 0.25% bupivacaine. Both regimens supported effective early postoperative analgesia, without compromising patient comfort or increasing the need for opioids.
Conclusion
This non-inferiority trial confirms that a 10 mL bolus of 0.15% bupivacaine is as effective as a 20 mL bolus of 0.25% bupivacaine when used for continuous adductor canal blocks in total knee arthroplasty. The two regimens delivered comparable pain relief, similar opioid requirements, and equivalent functional outcomes within the first 12 hours postoperatively.
The findings are particularly valuable in the context of regional anesthesia safety and efficiency. Using lower volumes and concentrations can reduce the total dose of local anesthetic, which may lower the risk of systemic toxicity, reduce drug costs, and simplify inventory management in high-volume surgical centers.
Importantly, the results support the idea that less can be more in regional anesthesia: with appropriate catheter placement and continuous infusion, small boluses are sufficient to maintain analgesia without compromising quality.
Future research
Future research should focus on determining whether the analgesic equivalence between the lower and higher bupivacaine doses persists beyond the initial 12-hour period and whether these regimens influence long-term functional recovery or patient satisfaction. Additional studies using imaging or neurophysiological assessments could provide deeper insights into block spread and duration, helping clarify the mechanisms behind the observed effectiveness.
Trials that compare various infusion rates or incorporate adjuvants like clonidine or dexmedetomidine may identify more efficient or longer-lasting regimens. Expanding investigations to different surgical populations, such as bilateral total knee arthroplasty or outpatient procedures, will test the broader applicability of these findings. Lastly, cost-effectiveness analyses should be conducted to evaluate the economic benefits of using reduced local anesthetic volumes and concentrations within ERAS protocols.
For more detailed information, refer to the full article in RAPM.
Kampitak W et al. Comparison of 10 mL 0.15% vs 20 mL 0.25% bupivacaine boluses for continuous adductor canal block in total knee arthroplasty: a randomized non-inferiority trial. Reg Anesth Pain Med. Published online May 20, 2025.
Download the Nerve Blocks App HERE for in-depth insights on the adductor canal block. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Block Manual Module on NYSORA360!