




Ensuring safe and effective fluid management in infants undergoing surgery is a critical concern in pediatric anesthesia. Balancing the risks of hypoglycemia, hyponatremia, and metabolic instability has long presented a challenge. A landmark prospective study published in the British Journal of Anaesthesia offers robust evidence that a balanced electrolyte solution containing 1% glucose is both effective and safe for intraoperative maintenance in infants.
Why this matters
Infants, due to their unique physiology, are particularly susceptible to intraoperative metabolic derangements:
- High basal metabolic rate
- Limited glycogen reserves
- Immature endocrine response
- Increased sensitivity to fluid shifts
Historically, concerns about hypoglycemia led to the liberal use of glucose-rich, often hypotonic, intravenous (IV) solutions. However, these practices introduced other risks, particularly hyponatremia and hyperglycemia, prompting a reevaluation of intraoperative fluid protocols.
The study at a glance
Conducted at two major Swedish centers – Karolinska University Hospital in Stockholm and Uppsala University Hospital – this large prospective observational study included 365 infants aged 1–12 months. All underwent surgery under general anesthesia with standardized administration of a 1% glucose-balanced electrolyte solution (Benelyte, Fresenius Kabi).
- Primary goal: Determine the incidence of intraoperative hypoglycemia.
- Secondary goals: Evaluate glucose, electrolyte, ketone, and acid-base balance.
Key characteristics:
- Age range: 1–12 months (mean 5.2 months)
- Exclusions: Prematurity <44 weeks PCA, metabolic disease, hepatic impairment
- Infusion rates: 3.97 mL/kg/h median (range: 4–8 mL/kg/h)
- Monitoring: Glucose every 30–60 minutes, full blood analysis pre- and post-anesthesia
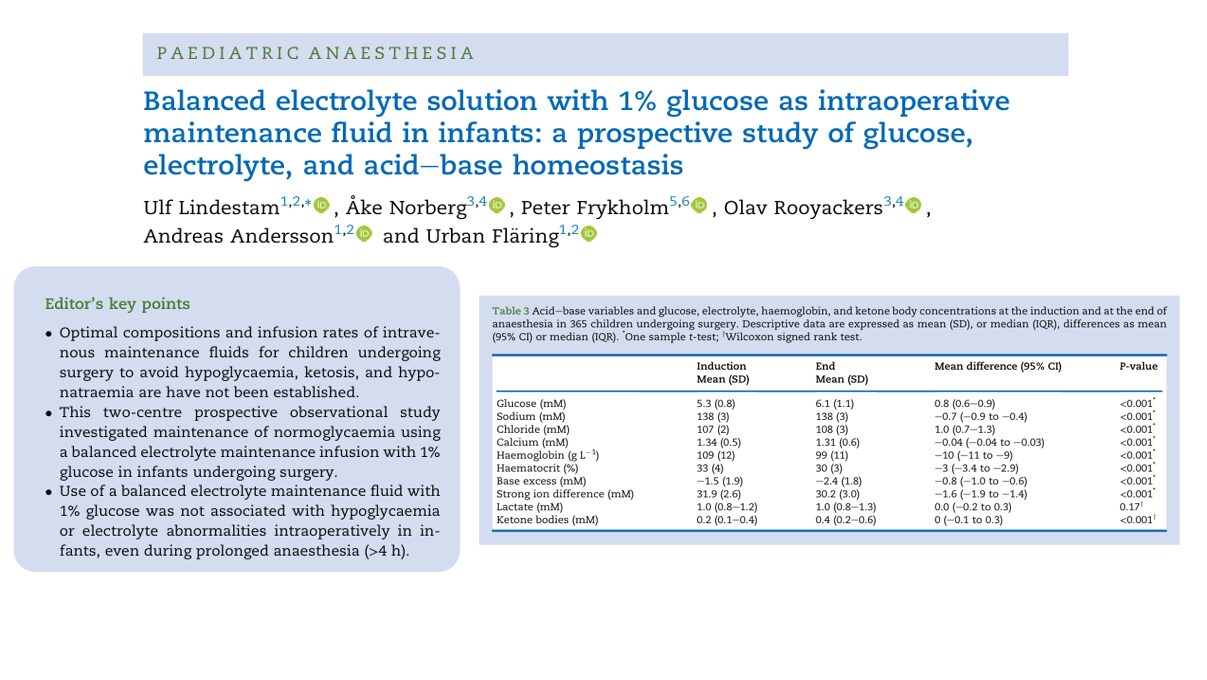
Main findings
- No cases of hypoglycemia
- Mean plasma glucose rose from 5.3 to 6.1 mM (p<0.001)
- No infant recorded glucose <3.0 mM
- Even among the youngest infants (≤3 months), levels remained stable or improved
- Mild hyperglycemia (>8.3 mM) was rare (4.3% of patients)
This result supports that 1% glucose is sufficient to maintain normoglycemia even with modest infusion rates and prolonged fasting.
- Sodium and chloride stayed within safe limits
- Mean sodium dropped slightly: 138 to 137.3 mM (p<0.001)
- Hyponatremia (<135 mM) rose slightly from 3.6% to 6.6%—but remained clinically insignificant
- Chloride increased from 107 to 108 mM, with 13.2% showing mild hyperchloremia at the surgery end
Infants receiving albumin boluses showed smaller sodium reductions, possibly due to their hypertonic properties.
- Acid-base and ketone trends remained mild
- Base excess (BE) declined from −1.5 to −2.4 mM, within a safe range
- Ketone levels increased modestly, particularly in surgeries >180 minutes
- No cases of dangerous acidosis or ketosis were recorded
Ketosis, a marker of fasting stress, remained largely within acceptable thresholds.
- Fasting did not significantly impact stability
Although 21% of infants fasted >6 hours, no association was found with adverse glucose or ketone trends.
- Median breastmilk/formula fast: 5 hours
- Only 12.3% received glucose-containing clear fluids pre-op
This suggests that adherence to updated fasting guidelines (6-4-1 rule) is generally safe when paired with appropriate fluid management.

Clinical implications
This study offers the strongest evidence to date supporting the intraoperative use of 1% glucose-balanced electrolyte fluids in infants. Its findings could lead to practice changes, including:
- Standardizing low-glucose, isotonic solutions in pediatric ORs
- Reducing unnecessary glucose supplementation
- Preventing avoidable complications such as cerebral edema from hyponatremia or hyperglycemia-induced immune impairment
Benefits of 1% glucose-balanced fluids
- Maintains metabolic and electrolyte stability
- Reduces risk of glucose and sodium disturbances
- Matches modern anesthetic practices (regional blocks, reduced fasting)
Step-by-step clinical protocol
- Pre-op screening
- Rule out metabolic or endocrine disease
- Confirm normal liver/kidney function
- Fasting prep
- Breastmilk: 4–6 hours
- Clear fluids: up to 1 hour pre-op
- Start infusion
- 4–8 mL/kg/h using 1% glucose-balanced solution
- Initial rate may be higher (10 mL/kg/h) to compensate for fasting
- Intraoperative monitoring
- Glucose: baseline, every 30–60 minutes
- Electrolytes and acid-base: at least at induction and end
- Adjust fluids or add boluses as needed
- Post-op reassessment
- Check glucose and sodium before full recovery
- Consider continued isotonic fluids if extended fasting is expected
Recommendations
For hospitals and anesthetists:
- Adopt balanced isotonic solutions with 1% glucose as standard for infants
- Train staff in correct dosing and monitoring protocols
- Phase out hypotonic high-glucose fluids to minimize sodium-related risks
For researchers:
- Investigate optimal fluid choices in special populations (preterms, neonates, endocrine disorders)
- Explore longer-term effects on recovery and neurological outcomes
Final thoughts
This comprehensive prospective study underscores a pivotal shift in pediatric anesthesia toward safer, smarter fluid choices tailored to the unique metabolic demands of infants. With compelling evidence that 1% glucose-balanced electrolyte solutions effectively safeguard against intraoperative hypoglycemia and electrolyte imbalance, clinicians have a validated, evidence-backed foundation for updating protocols.
For more detailed information, refer to the full article in British Journal of Anaesthesia
Reference: Lindestam U, Norberg Å, Frykholm P, Rooyackers O, Andersson A, Fläring U. Balanced electrolyte solution with 1% glucose as intraoperative maintenance fluid in infants. Response to Br J Anaesth 2025; 135: 798-9. Br J Anaesth.
For more literature updates in pediatric anesthesia, read NYSORA’s Pediatric Anesthesia Updates 2025!