
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
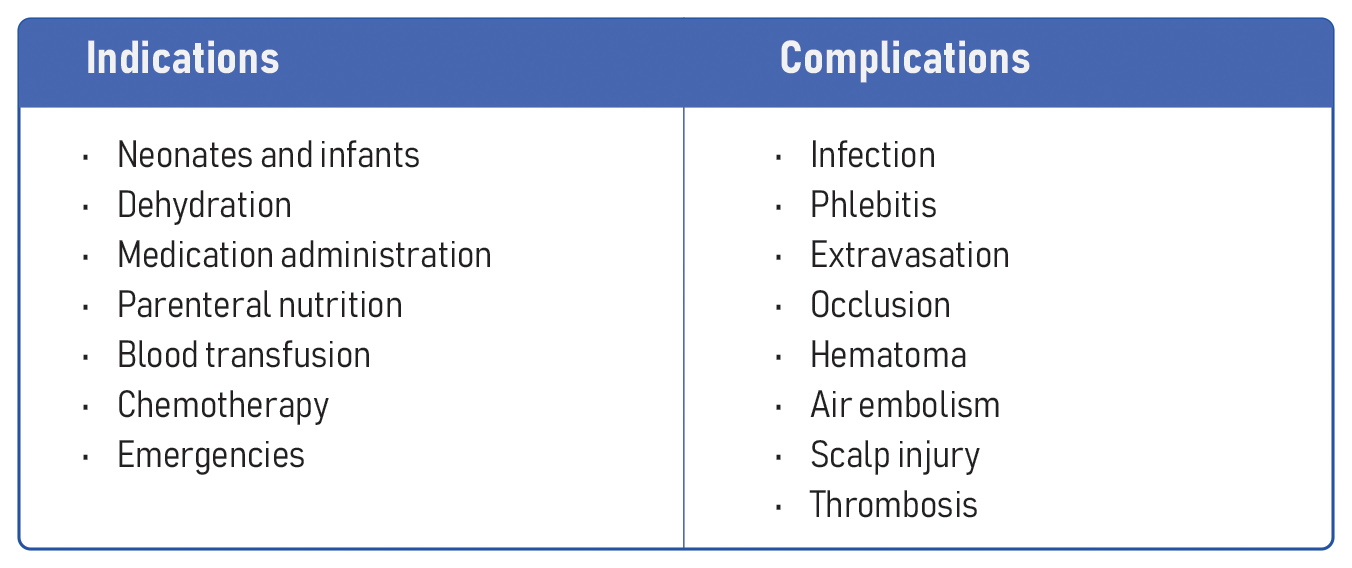
Securing venous access in infants and children presents unique challenges due to the delicate nature of their veins, potential dehydration, and anxiety about the procedure. This manual focuses primarily on IV access in adults. However, here are essential points to consider when attempting vein access in pediatric patients.
Smaller and fragile veins
- Challenge: The veins of pediatric patients are notably smaller and more fragile than those of adults, requiring extra care and precision during venipuncture.
- Solution: Choose the smallest IV gauge that meets the needs of the prescribed therapy to minimize discomfort and potential damage to veins.
- Note: Ultrasound can be used to aid the vein identification and cannulation. However, ultrasound-guided IV insertion is typically best reserved for challenging cases as it requires additional equipment, time, and expertise and is not suited for small, superficial veins, which is the case for most pediatric patients.
Movement concerns
- Challenge: Children frequently move during cannulation, which increases the risk of catheter dislodgement.
- Solution: In particularly challenging scenarios, such as with uncooperative children or patients with certain disabilities who require IV access, consider the administration of intramuscular ketamine (2-4 mg/kg). This creates a state of sedation and transient amnesia within approximately 5-10 minutes, providing a window of opportunity to insert a catheter or draw blood for analysis. Properly secure and stabilize the catheter after insertion, and consider using pediatric-specific securement devices to accommodate children’s activity levels.
Discomfort
- Challenge: The process of IV insertion can be a source of significant discomfort and distress for children, complicating the procedure.
- Solution: Use soothing strategies such as offering infants pacifiers or distraction methods. Manage pain proactively by applying topical anesthetics to the intended insertion site to numb this area.
Vein selection
- Challenge: Determining the most suitable venipuncture site can be challenging due to children’s smaller, less visible, or less palpable veins.
- Solution: Consider the more accessible scalp veins or foot veins in neonates.
Surface veins in neonates
- Challenge: In neonates and newborns, veins lie very close to the skin’s surface, making them more susceptible to being punctured through and making venipuncture challenging.
- Solution: During insertion, maintain the needle at a very low, almost flat angle, nearly parallel to the skin. This technique allows for better control of the depth of needle entry, reducing the risk of puncturing the opposite vein wall or causing tissue trauma.

Foot veins may be used for IV access in pediatric patients as they may be more accessible than the standard peripheral veins in the arm or hand.
VIDEO: https://youtu.be/p9XKRftTeTM
Step-by-step technique of IV cannulation in the hand of a pediatric patient






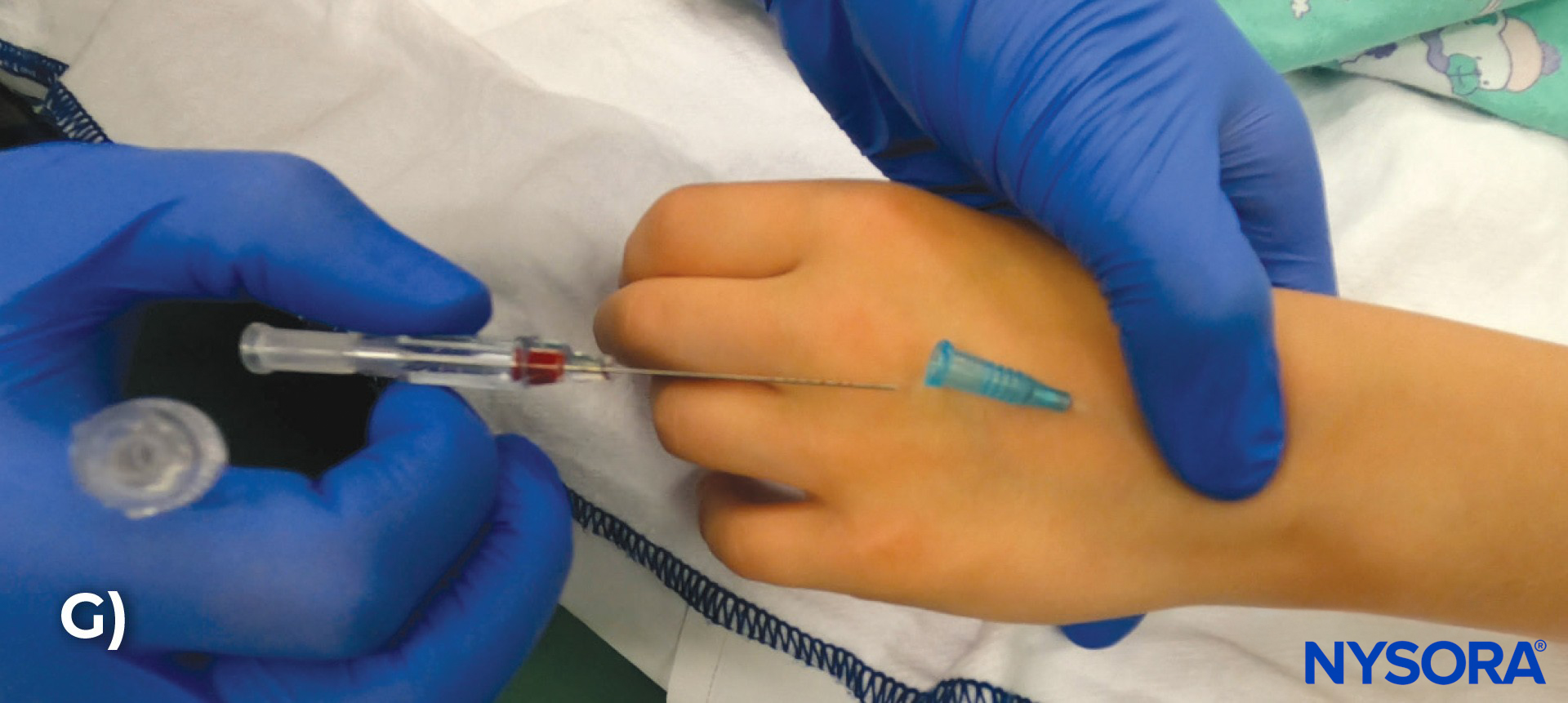
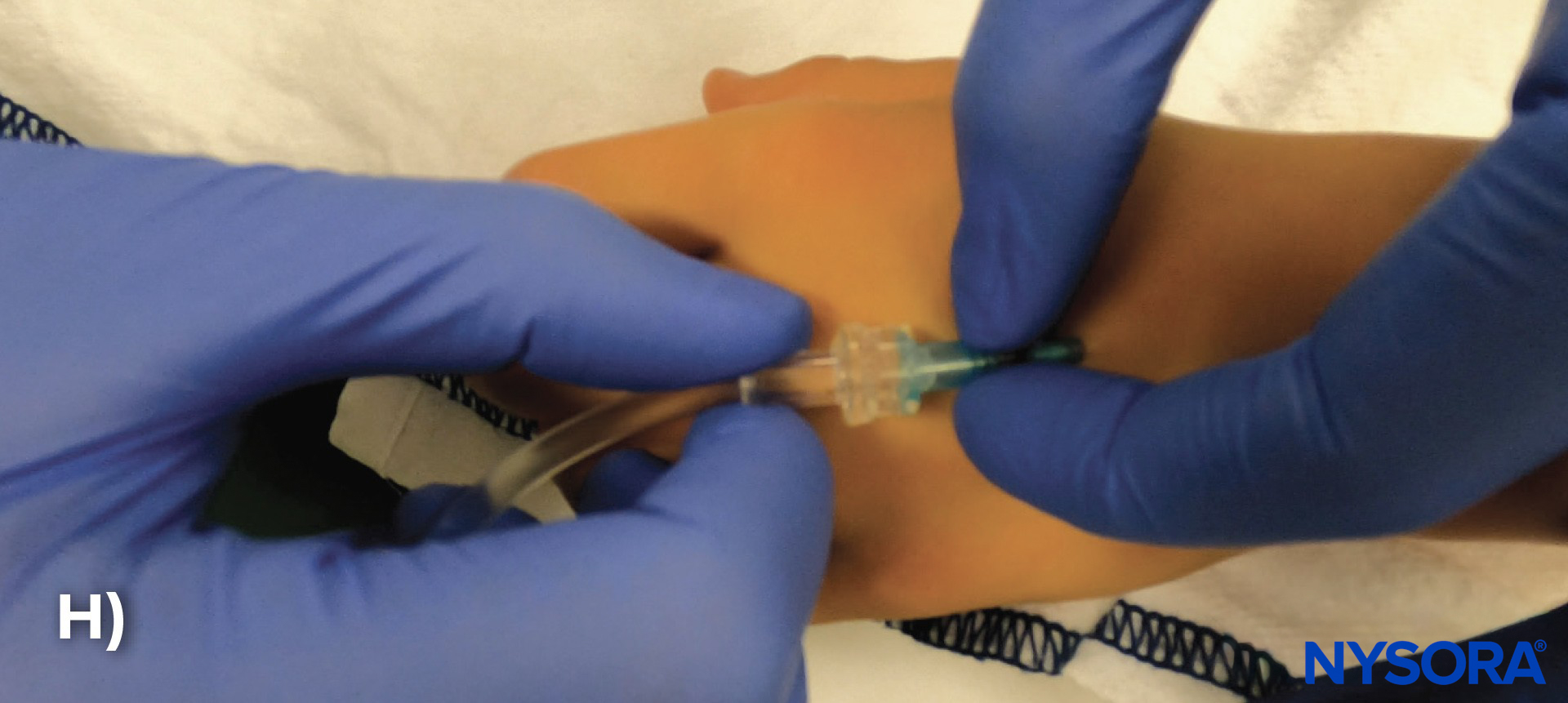


A) Disinfect the insertion site. B) Stabilize the veins in the hand and select a vein. C) Insert the needle at a shallow angle of 15-30 degrees relative to the skin. D) Blood in the flashback chamber indicates that the needle is inside the vein. E) Advance the catheter an additional 1-2 mm to ensure that the catheter tip is in the vein. F) Thread the catheter over the needle into the vein. G) Retract the needle. H) Attach the IV tubing to the catheter. I) Secure the catheter with an occlusive dressing. J) Loop the IV tubing and tape it to the skin away from the insertion site.
TIPS
- Catheter size: Select the optimal catheter gauge. A short 24G or 26G catheter is typically the best in pediatric patients. To put the flow rates in perspective, using a 24G IV in an infant is equivalent to using two 18G IVs in adults.
- Site preference: The best anatomical IV insertion sites are often the back of the hand in children or feet in babies.
- In babies and small children, securing a vein in the foot is often easier since the hand is more prone to movement. Transillumination is a valuable tool to pinpoint veins in the dorsum of the hand.
- Immobilize: The key to successful IV insertion in infants is immobilizing the extremity where the IV is placed. The tendency of children to wiggle can render IV insertion nearly impossible.
- Use the free hand: Use your free hand to stabilize the vein, pull the skin away, and immobilize the hand while starting an IV line with the other hand.
VIDEO: https://youtu.be/8W7DA2KHwPM
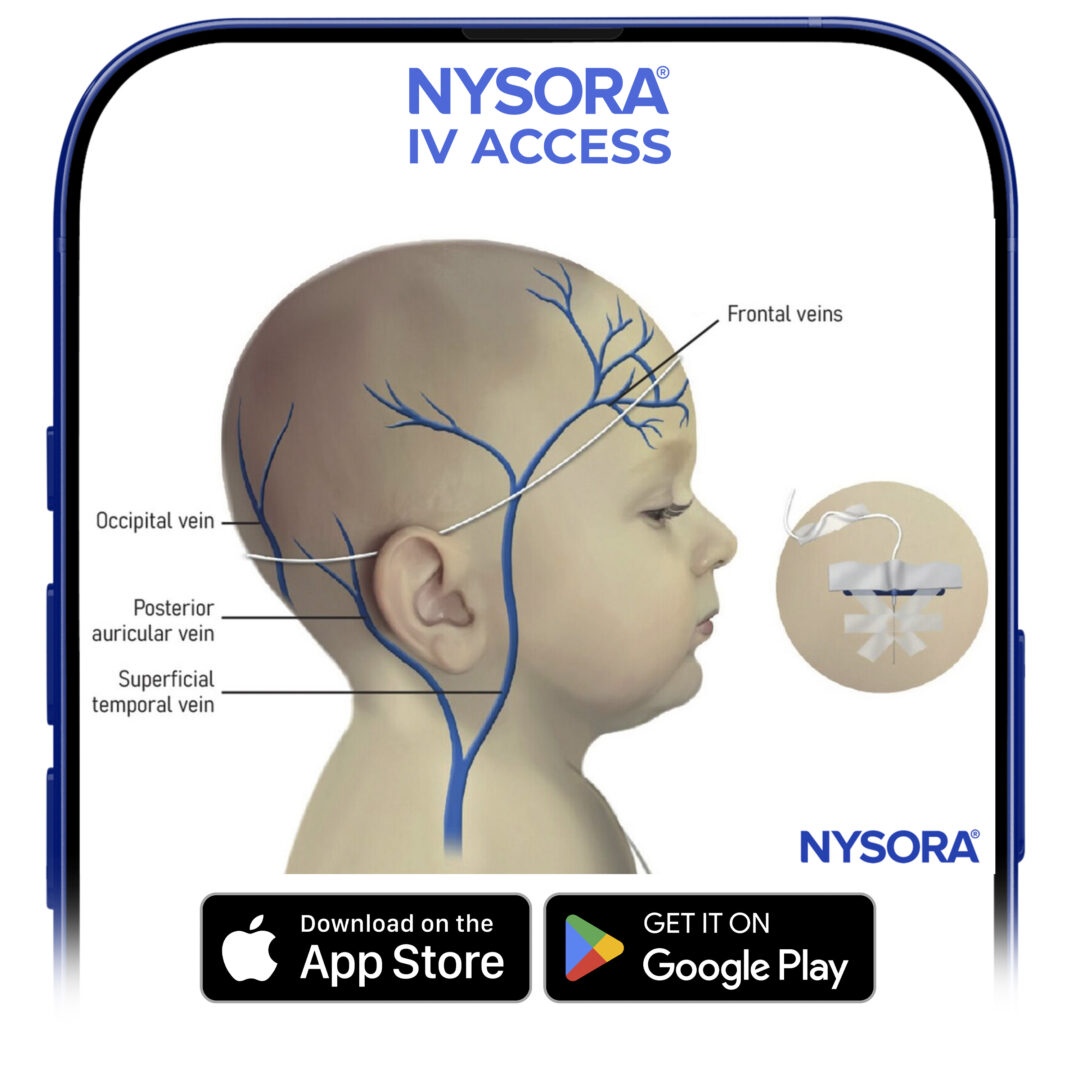
Scalp vein cannulation
Scalp vein cannulation, often utilized in infants and young children, is an alternative for peripheral IV access when traditional venous access in the arms or legs is challenging. It can also be used in adults under similar circumstances.
Here are some tips for effective scalp vein cannulation.
Patient preparation: Explain the procedure to parents or guardians and ensure the child is as comfortable as possible.
Patient position: Gently restrain the infant’s head or ask an assistant to hold it steady. A calm, soothing environment helps in keeping the child relaxed.
Vein selection: Scalp veins are generally more prominent and accessible in neonates and infants. Choose a vein that appears straight and well-distended.
Use of a smaller gauge needle: Select a smaller gauge butterfly needle, which is more suitable for the scalp veins. Use a 24G or 26G butterfly needle to insert the IV catheter at a 20-30 degree angle.
Sterile technique: Clean the chosen site with an antiseptic solution and maintain an aseptic technique throughout the procedure.
Gentle insertion: Carefully insert the needle at a low angle, with the bevel facing up. The scalp’s superficial veins require a delicate touch to avoid puncturing the vein.
Secure the cannula: Once in place, secure the needle with tape, ensuring it doesn’t obstruct the child’s movements or cause discomfort.
Use of protective covering: Consider using a soft, protective covering over the site to prevent accidental dislodgement.
Regular monitoring: Frequently check the IV site for signs of infiltration, infection, or phlebitis, especially since the pediatric patient may be unable to communicate discomfort effectively.
Pain management: Minimize discomfort during the procedure with appropriate pain management strategies.
Documentation: Record the procedure details including the cannulation site, the needle size, and any complications or patient reactions.
Parental guidance: Provide parents or guardians with information on how to care for the IV site and what signs of complications to look for.
Scalp vein cannulation requires skill and patience and should be performed by healthcare professionals experienced in pediatric IV therapy. The primary focus should always be on patient safety and comfort.

Scalp vein cannulation, often utilized in infants and young children, is an alternative for peripheral IV access when traditional venous access in the arms or legs is challenging.
Pediatric cerebral palsy patient
Video: https://youtu.be/l55PoOYNRDA
Video: https://youtu.be/tXIiiw-qip8
Clinical updates
- Charters et al. (JAMA Pediatrics, 2024) conducted a 3-arm randomized trial showing that securing pediatric peripheral IV catheters with an integrated securement dressing plus tissue adhesive reduced overall catheter failure from 34% (standard bordered polyurethane dressing) to 12%, primarily by decreasing unintentional dislodgement. Importantly, despite slightly higher upfront product costs, total hospital costs were lower with integrated securement plus adhesive due to fewer failures and reinsertion needs, with similar pain scores, dwell times, and staff/caregiver satisfaction.
Reference: Charters B et al. Novel Peripheral Intravenous Catheter Securement for Children and Catheter Failure Reduction: A Randomized Clinical Trial. JAMA Pediatr. 2024;178:437-445.
- Akgül et al. (Journal of Pediatric Nursing, 2024) conducted a randomized controlled trial evaluating a soft therapeutic toy (“Comfie”) during neonatal IV cannula insertion and found significantly improved physiologic stability and comfort compared with standard care. During insertion, the Comfie group had lower pulse and higher oxygen saturation, and at 1–5 minutes post-procedure, maintained lower pulse and respiratory rates with higher saturation; comfort scores were better, and crying time was nearly halved. The intervention demonstrated large clinical effect size and suggests that simple toy-based distraction may be an effective nonpharmacologic strategy to improve neonatal comfort and physiologic stability during IV placement.
Reference: Akgül EA et al. The effectiveness of the therapeutic toys on the comfort level and vital signs of the neonates during intravenous cannula insertion (Comfiestudy): A randomized controlled trial. J Pediatr Nurs. 2024;76:e27-e33.
- Heydinger et al. (Pediatric Health, Medicine and Therapeutics, 2022) conducted a prospective observational study of 1002 children undergoing anesthesia and found that 9% met criteria for difficult IV access, with 78% successful on the first attempt and 91% within two attempts. Independent predictors of DIVA included age < 1 year, age 1–3 years, ASA II status, and prior history of difficult IV placement, while BMI, race, gender, provider type, and induction technique were not significant predictors. These findings support early identification of younger, higher-ASA, and previously difficult patients to consider escalation strategies in the perioperative setting.
Reference: Heydinger G et al. Characterization of the Difficult Peripheral IV in the Perioperative Setting: A Prospective, Observational Study of Intravenous Access for Pediatric Patients Undergoing Anesthesia. Pediatric Health Med Ther. 2022;13:155-163.











