
Learning objectives
- Describe the causes of and risk factors for increased intracranial pressure
- Identify increased intracranial pressure
- Manage increased intracranial pressure
Background
- Increased intracranial pressure (ICP) commonly occurs in patients with traumatic brain injury and subarachnoid hemorrhage
- It is the most frequent cause of morbidity and mortality in these patients
- Brain tumors can also increase ICP
- Increased ICP can impair cerebral perfusion pressure, cerebral blood flow, and cerebral oxygenation, resulting in ischemia, edema, and further increases in ICP
- Can impede surgical access to deep lesions requiring brain retraction
- Can predispose to or exacerbate brain retraction injury
- Can complicate dural closure
Signs
- Before craniotomy:
- Hypertension
- Bradycardia
- Irregular respiratory pattern (Cushing reflex)
- After craniotomy:
- Tense dura
- Brain swelling out of the dural opening
- Difficult brain retraction
- Quantitative measurements:
- ICP monitoring (External ventricular drain, intraparenchymal pressure monitor)
- ICP measurement (Pressure transducer slid into the epidural space from a burr hole or at the edge of a craniotomy)
Risk factors
- Subdural ICP >10 mmHg
- Peritumoral edema
- Mean arterial blood pressure >140 mmHg
- Intraoperative hypotension with systolic blood pressure <90 mmHg
- Glioblastoma
- Metastasis
Causes
- Intracranial
- Tumor
- Infarct
- Trauma
- Hemorrhage
- Hydrocephalus
- abscess/infection
- Parenchymal edema
- Idiopathic
- Extracranial
- Airway obstruction
- Hypoxia/hypercarbia
- Hypertension exceeding cerebral autoregulatory capacity
- Hypotension causing cerebral hypoperfusion and reflex vasodilation
- Venous hypertension from outflow obstruction
- Volatile anesthetics
- Nitroglycerin
- Sodium nitroprusside
- Vomiting, coughing, pain, shivering, and seizure activity during awake craniotomy
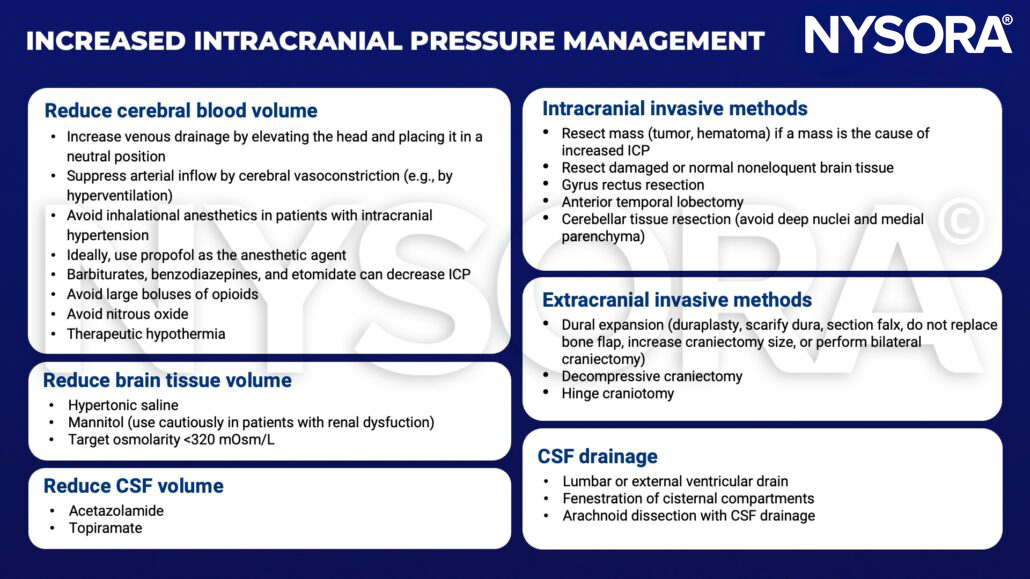
Management
Suggested reading
- Desai VR, Sadrameli SS, Hoppe S, Lee JJ, Jenson A, Steele WJ, et al. Contemporary Management of Increased Intraoperative Intracranial Pressure: Evidence-Based Anesthetic and Surgical Review. World Neurosurgery. 2019;129:120-9.
- Ragland J, Lee K. Critical Care Management and Monitoring of Intracranial Pressure. J Neurocrit Care. 2016;9(2):105-12.
- Tameem A, Krovvidi H. Cerebral physiology. Continuing Education in Anaesthesia Critical Care & Pain. 2013;13(4):113-8.
Clinical updates
Diz et al. (Anesthesia & Analgesia, 2025) report in a meta-analysis of 15 RCTs (>35,000 patients) that balanced crystalloids are associated with higher mortality in traumatic brain injury, likely related to increased cerebral edema and intracranial pressure, whereas non-TBI patients benefited from balanced solutions. These findings support preferential use of normal saline in patients at risk of elevated ICP, reinforcing diagnosis-specific fluid selection in neurocritical care.
- Read more about this study HERE.











