Explore NYSORA knowledge base for free:
Explore NYSORA knowledge base for free:

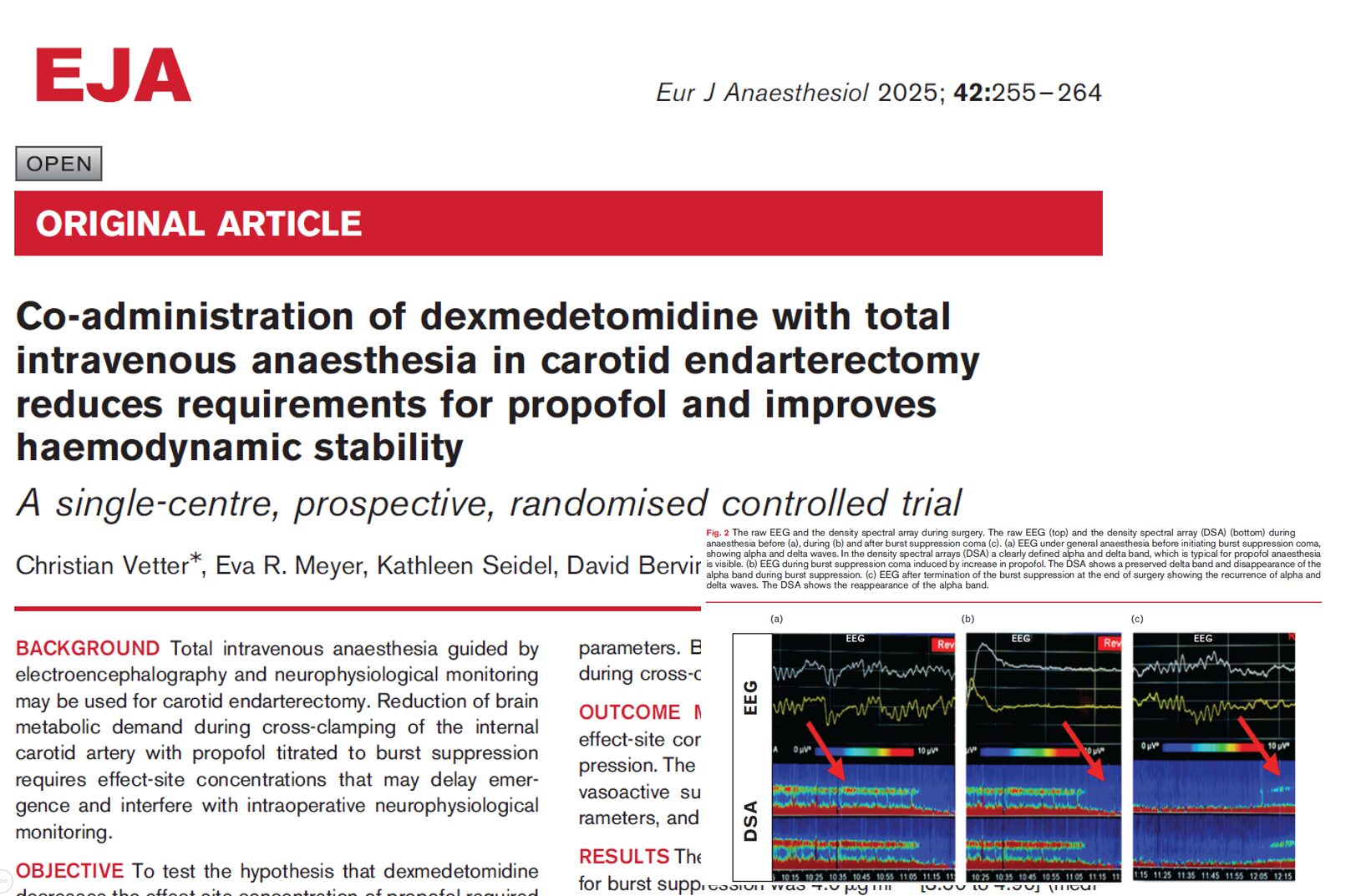
A new randomized controlled trial by Vetter et al. published in the European Journal of Anaesthesiology (2025) sheds light on the significant benefits of combining dexmedetomidine with total intravenous anesthesia (TIVA) in patients undergoing carotid endarterectomy (CEA). Conducted at the University Hospital of Bern, Switzerland, this single-center trial demonstrates that dexmedetomidine not only reduces propofol requirements but also improves hemodynamic stability without compromising neurophysiological monitoring or recovery. Key findings at a glance Reduction in Propofol requirements: Dexmedetomidine lowered the propofol effect-site concentration required for burst suppression by 33%. Improved hemodynamic stability: Patients receiving dexmedetomidine required 50% less norepinephrine to maintain target blood pressures. Preservation of neurophysiology: No significant adverse effects on intraoperative somatosensory (SEP) or motor-evoked potentials (MEP). No increase in postoperative delirium: Cognitive recovery and delirium rates were comparable between groups. Background: Why Dexmedetomidine? CEA is a surgical procedure to reduce the risk of stroke in patients with internal carotid artery (ICA) stenosis. General anesthesia (GA), particularly TIVA with propofol, is often preferred to facilitate intraoperative neurophysiological monitoring (IONM). However, inducing burst suppression (BS) with propofol to lower cerebral metabolic demand often requires high doses, resulting in: Increased vasopressor needs Hemodynamic fluctuations Delayed emergence Dexmedetomidine, an alpha-2 adrenergic agonist, has shown promise for: Reducing anesthetic requirements Stabilizing blood pressure Offering potential neuroprotective effects Study design and methods Inclusion criteria: ASA physical status ≤ 4 Symptomatic/asymptomatic ICA stenosis Age ≥ 18 years Exclusion criteria: Significant cardiac arrhythmias, bradycardia, severe hypovolemia Liver disease, known propofol/dexmedetomidine hypersensitivity Pregnancy, cardiovascular instability, limited autonomic activity Dexmedetomidine group: Bolus: 0.4 µg/kg over 10 minutes before induction Infusion: 0.4 µg/kg/h until surgical closure Control group: Standard TIVA without dexmedetomidine Both groups: Propofol administered via target-controlled infusion (TCI) Titrated to achieve EEG burst suppression (verified via raw EEG and spectral analysis) Remifentanil and fentanyl for analgesia Normoventilation […]
New York City—where tradition meets tomorrow—is setting the stage for an electrifying convergence of minds and ideas. In the heart of Times Square, NYSORA is redefining the art and science of anesthesia with an event that’s as innovative as it is international. What’s On the Program? Master the Complex: Tackle high-risk cases, from obesity and OSA challenges to breakthrough orthopedic procedures. Stay on the Cutting Edge: Dive into the latest in opioid-free anesthesia, fluid resuscitation breakthroughs, and revolutionary high-flow nasal cannula techniques. Embrace the Future: See firsthand how AI, machine learning, and advanced ultrasound techniques are reshaping anesthetic safety and efficiency. Champion Wellness & Sustainability: Explore strategies to shrink anesthesia’s carbon footprint, fight burnout with biohacking, and discover pioneering approaches to pain management and longevity. Elevate Your Expertise: Gain hands-on experience with advanced nerve block techniques, spinal anesthesia innovations, and more—bringing transformative skills back home. At its 18th edition, the NYSORA Symposium isn’t just an event—it’s the birthplace of the future of anesthesiology. Join us at the Sheraton in Times Square from September 26-28, 2025. Secure your spot now and be part of the revolution in anesthesia. Who else but NYSORA calls NYC home? Register Today.

Total hip arthroplasty (THA) is a frequently performed surgical procedure to improve mobility and quality of life in patients with advanced hip joint disease. However, significant postoperative pain is a common challenge and can hinder recovery, delay rehabilitation, and increase opioid consumption. Multimodal analgesia, incorporating a combination of systemic and regional techniques, has become the cornerstone of postoperative pain management in THA. The anterior quadratus lumborum block (QLB) has emerged as a potential technique for addressing the complex innervation of the hip joint. This multicenter, randomized, placebo-controlled trial evaluated whether adding anterior QLB to multimodal analgesia improves postoperative outcomes in patients undergoing THA. Study objective and methods The study aimed to assess the impact of anterior QLB on postoperative pain, opioid consumption, and functional recovery in THA patients. Design: Multicenter, randomized, double-blind, placebo-controlled trial. Participants: 60 patients undergoing primary unilateral THA were randomized to receive either anterior QLB with 20 mL of 0.2% ropivacaine (n = 30) or a placebo saline injection (n = 30). Intervention: Anterior QLB was performed preoperatively with ultrasound guidance, injecting local anesthetic or saline between the quadratus lumborum and psoas major muscles. Both groups received multimodal analgesia, including NSAIDs, acetaminophen, ketamine, and dexamethasone. Primary outcome: Cumulative opioid consumption (oral morphine equivalents) in the first 24 hours postoperatively. Secondary outcomes: Pain scores, time to first standing, walking distance, quadriceps strength, and 3-month functional recovery metrics. Key findings Opioid consumption: There was no significant difference in cumulative opioid consumption between the QLB and placebo groups. Median opioid use in the first 24 hours was 40 mg (IQR 20–50 mg) for the QLB group and 31 mg (IQR 20–45 mg) for the placebo group (P = 0.6). Pain scores: Pain intensity was similar between the two groups at all measured time points. The QLB group did not […]