Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About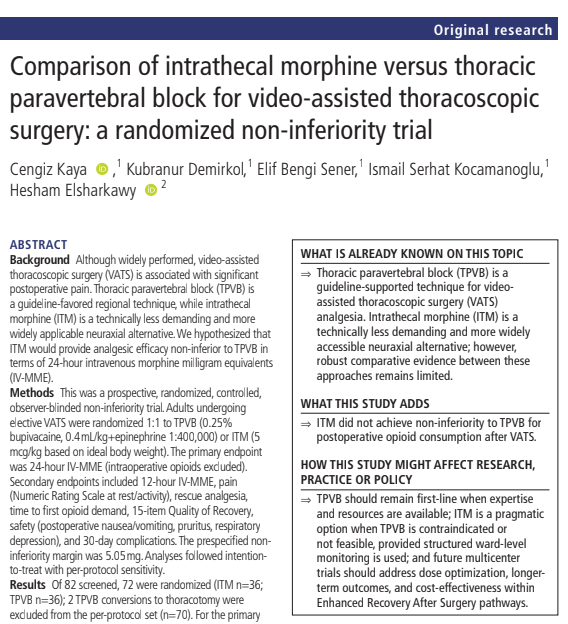





Thoracic paravertebral block remains the preferred regional analgesic technique for video-assisted thoracoscopic surgery, according to a new randomized non-inferiority trial. While intrathecal morphine provided comparable pain scores and recovery quality, it failed to demonstrate non-inferiority for reducing postoperative opioid consumption, reinforcing current guideline recommendations.
Video-assisted thoracoscopic surgery still presents a significant pain management challenge
Video-assisted thoracoscopic surgery (VATS) has transformed thoracic surgery by reducing tissue trauma, shortening hospital stays, and accelerating postoperative recovery compared with open thoracotomy. Nevertheless, postoperative pain remains a major clinical concern.
Moderate-to-severe pain affects nearly two-thirds of patients undergoing VATS. Poorly controlled pain impairs coughing, deep breathing, sputum clearance, and early mobilization while increasing the risk of pulmonary complications and chronic postsurgical pain.
Modern Enhanced Recovery After Surgery (ERAS) pathways emphasize multimodal analgesia, combining systemic medications with regional anesthesia techniques to minimize opioid exposure while maintaining excellent pain control.
Among available regional techniques, thoracic paravertebral block (TPVB) is widely recommended. However, intrathecal morphine (ITM) offers several practical advantages, including technical simplicity, single-shot administration, and broad availability in hospitals where ultrasound-guided regional anesthesia expertise may be limited.
Until now, robust head-to-head evidence comparing these two strategies has been limited.
New randomized trial compares two commonly used analgesic techniques
Researchers conducted a prospective randomized observer-blinded non-inferiority trial evaluating postoperative analgesia after elective VATS.
Study design
The investigators enrolled:
- 72 adult patients undergoing elective VATS
- ASA physical status I–III
- Randomized 1:1
- 36 patients received thoracic paravertebral block
- 36 patients received intrathecal morphine
Two patients converted from VATS to thoracotomy and were excluded from the per-protocol analysis.
Regional anesthesia protocols
Thoracic paravertebral block
- Ultrasound-guided
- T5 level
- 0.25% bupivacaine
- Epinephrine added
Intrathecal morphine
- Lumbar spinal injection
- Morphine dose:
- 5 μg/kg
- Based on ideal body weight
All patients received identical general anesthesia, multimodal postoperative analgesia, and morphine patient-controlled analgesia (PCA).
Primary outcome focused on opioid consumption
Rather than simply comparing pain scores, investigators selected a clinically meaningful primary endpoint:
Total intravenous morphine milligram equivalents (IV-MME) during the first 24 postoperative hours.
The study was designed as a non-inferiority trial, asking whether intrathecal morphine could provide analgesia that was not clinically worse than thoracic paravertebral block.
The predefined non-inferiority margin was:
5.05 mg IV morphine equivalent.
Intrathecal morphine did not achieve non-inferiority
The primary analysis demonstrated that intrathecal morphine failed to meet the prespecified non-inferiority criterion.
Intention-to-treat analysis
Median difference (ITM − TPVB):
- 6.5 mg IV-MME
- 95% confidence interval:
- 1–17 mg
Because the upper confidence interval exceeded the predefined non-inferiority margin, investigators concluded that intrathecal morphine could not be considered non-inferior.
The findings remained consistent in the per-protocol analysis.
Thoracic paravertebral block reduced opioid requirements
Patients receiving thoracic paravertebral block consistently required fewer opioids throughout the first postoperative day.
Median opioid consumption
12 hours
- ITM:
- 17 mg IV-MME
- TPVB:
- 4.5 mg
24 hours
- ITM:
- 21.5 mg
- TPVB:
- 7 mg
These differences were statistically significant.
In addition, significantly more patients receiving intrathecal morphine required rescue analgesics during the first 24 hours.
Pain scores remained remarkably similar
One of the study’s most interesting findings is that lower opioid consumption did not translate into significantly different patient-reported pain scores.
Investigators measured pain:
- At rest
- During coughing or deep breathing
- At multiple postoperative time points
Across all assessments:
- Resting pain scores were similar.
- Activity pain scores were similar.
- Overall pain trajectories did not differ significantly.
This suggests that both techniques produced acceptable analgesia, although patients receiving intrathecal morphine required more supplemental opioids to achieve comparable comfort.
Recovery quality was nearly identical
Beyond pain control, investigators assessed postoperative recovery using the validated Quality of Recovery-15 (QoR-15) questionnaire.
The questionnaire evaluates:
- Physical comfort
- Emotional state
- Pain
- Independence
- Psychological support
QoR-15 scores were comparable:
- Before surgery
- At 24 hours
- At hospital discharge
Therefore, despite greater opioid requirements, intrathecal morphine did not appear to negatively influence overall patient recovery.
Safety outcomes were reassuring
A common concern with intrathecal morphine is delayed respiratory depression due to rostral spread within cerebrospinal fluid.
Importantly, investigators observed:
- No postoperative respiratory depression
- Similar postoperative nausea and vomiting rates
- Mild pruritus only in a small number of ITM patients
- No major neurological complications
- No clinically significant safety concerns
All recorded 30-day postoperative complications were classified as Clavien-Dindo Grade I, representing minor postoperative events.
These findings support previous evidence suggesting that low-dose intrathecal morphine (≤5 μg/kg) can be administered safely with structured postoperative monitoring.
Why did thoracic paravertebral block perform better?
The difference likely reflects the distinct pharmacology and mechanisms of action.
Thoracic paravertebral block
TPVB provides:
- Immediate segmental sensory blockade
- Unilateral thoracic analgesia
- Sympathetic blockade
- Excellent early postoperative pain control
Because the local anesthetic begins working immediately, opioid requirements are reduced during the period when pain is often greatest.
Intrathecal morphine
Intrathecal morphine behaves differently.
Morphine is highly hydrophilic, meaning it spreads slowly within cerebrospinal fluid.
Consequently:
- Analgesia develops gradually
- Peak effect occurs several hours after injection
- Early postoperative pain may require additional systemic opioids
This delayed onset likely explains why patients receiving ITM consumed more opioids despite eventually reporting pain scores similar to those receiving TPVB.
Clinical implications for anesthesiologists
The findings reinforce current international recommendations favoring thoracic paravertebral block for VATS whenever expertise and resources are available.
According to the study, TPVB offers:
- Lower postoperative opioid consumption
- Reduced need for rescue analgesics
- Comparable pain control
- Similar recovery quality
- Excellent safety profile
However, the investigators also emphasize that intrathecal morphine remains an important alternative.
Hospitals without routine ultrasound-guided regional anesthesia programs may find ITM attractive because it:
- Is technically straightforward
- Requires minimal equipment
- Can be performed rapidly
- Provides prolonged analgesia
When used appropriately, structured ward monitoring, including continuous pulse oximetry and routine sedation assessment, can help ensure patient safety.
Key takeaways
- Thoracic paravertebral block remains the preferred regional analgesic technique for VATS.
- Intrathecal morphine failed to demonstrate non-inferiority for 24-hour postoperative opioid consumption.
- TPVB significantly reduced opioid requirements and rescue analgesic use.
- Patient-reported pain scores and quality of recovery were similar between groups.
- No postoperative respiratory depression occurred with low-dose intrathecal morphine under structured monitoring.
- Intrathecal morphine remains a pragmatic alternative when TPVB cannot be performed.
- Future multicenter studies should refine dosing strategies, evaluate long-term outcomes, and explore cost-effectiveness.
Reference: Kaya C et al. Comparison of intrathecal morphine versus thoracic paravertebral block for video-assisted thoracoscopic surgery: a randomized non-inferiority trial. Reg Anesth Pain Med. Published online June 17, 2026.
Download the Nerve Blocks App HERE for instant access to step-by-step guidance on the paravertebral block and other regional anesthesia techniques. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format – an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!