




Minimally invasive spine procedures are gaining traction as safer, effective alternatives to traditional open surgery for lumbar disc herniation. A newly published study in Pain Medicine (2025) delivers promising data on percutaneous laser disc decompression (PLDD), a technique that uses focused laser energy to reduce disc pressure and size, leading to both structural and symptomatic improvement.
Understanding lumbar disc herniation
Lumbar disc herniation occurs when the nucleus pulposus, the soft, gel-like center of an intervertebral disc, bulges or leaks through a tear in the outer ring (annulus fibrosus). This herniation can compress nearby nerve roots, leading to low back pain, radicular leg pain (sciatica), numbness, or weakness.
Key features:
- Most commonly occurs at L4-L5 and L5-S1 levels
- Affects adults aged 30–60
- Often results from age-related disc degeneration
- Typically begins with conservative treatment (e.g., physical therapy, NSAIDs, epidural injections)
While many herniations resolve on their own, a subset of patients fail conservative therapy and may require surgical intervention.
What is percutaneous laser disc decompression (PLDD)?
PLDD is a minimally invasive spinal procedure that uses laser energy to vaporize part of the herniated disc. By reducing the intradiscal pressure, PLDD alleviates compression on nearby nerve roots, reducing pain and restoring function.
Procedure overview:
- Done under local anesthesia with sedation
- Laser introduced via a spinal needle
- Performed under fluoroscopic guidance
- No sutures; typically an outpatient procedure
- Patients resume activity by day 2
The laser used is a 1470 nm diode, calibrated to deliver 800 joules in controlled bursts, allowing precise and safe ablation of nucleus pulposus tissue.
The study: methodology and patient profile
This retrospective study, conducted between January 2022 and April 2024, evaluated 58 patients who underwent PLDD for single-level, contained lumbar disc herniation.
Inclusion criteria:
- Persistent radicular pain despite 4+ months of conservative treatment
- Confirmed contained disc protrusion on MRI (not extruded or sequestered)
- Minimal neurologic deficits (motor strength ≥ 4/5)
Exclusion criteria:
- Previous lumbar surgery
- Severe spinal stenosis
- Disc height reduction >50%
- Extruded/sequestered discs or foraminal bony stenosis
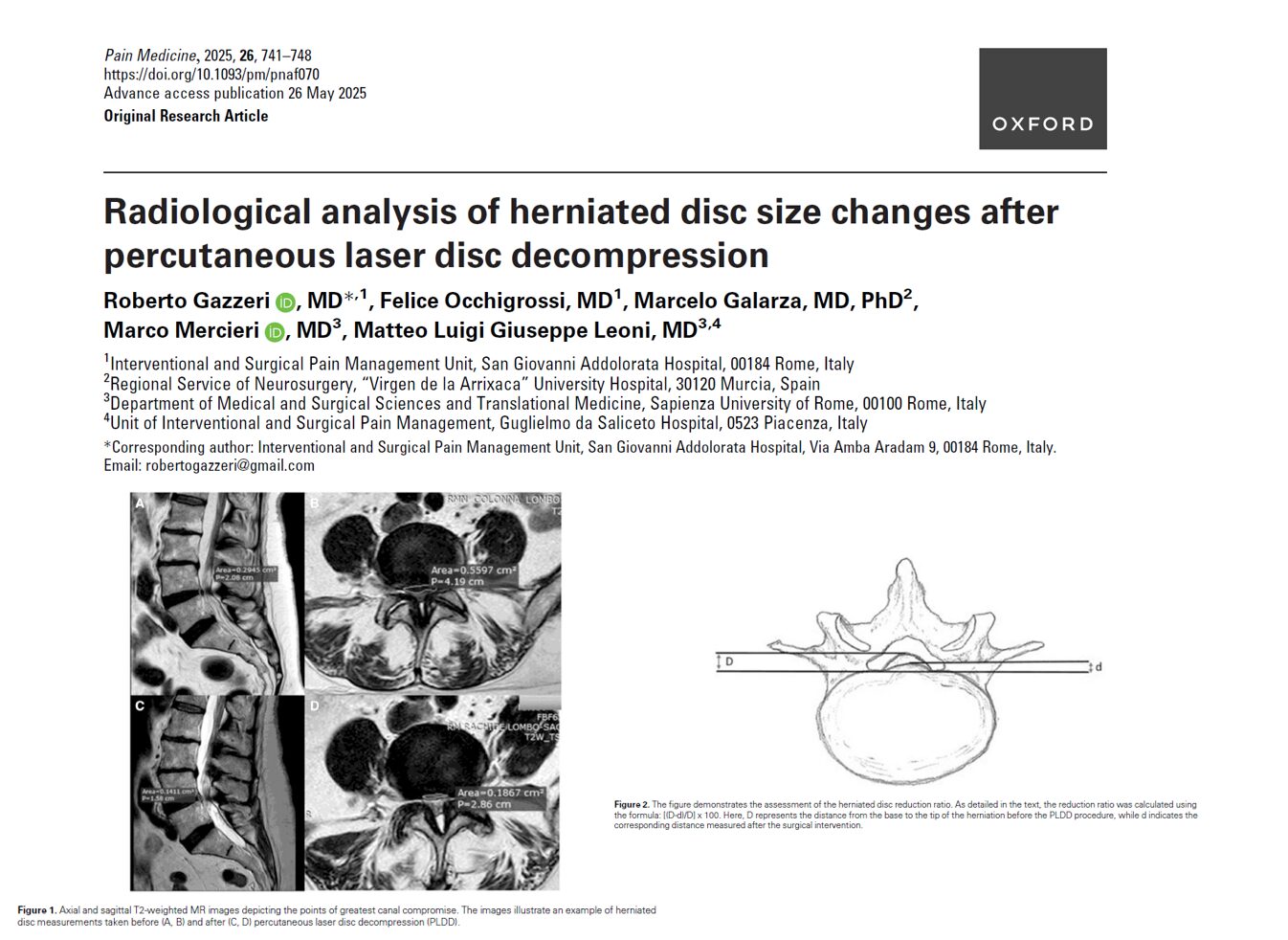
The study measured disc area on preoperative and 2-month postoperative MRI scans, both in axial and sagittal planes, using specialized radiology software (RadiAnt DICOM Viewer).
Radiological outcomes: significant disc shrinkage
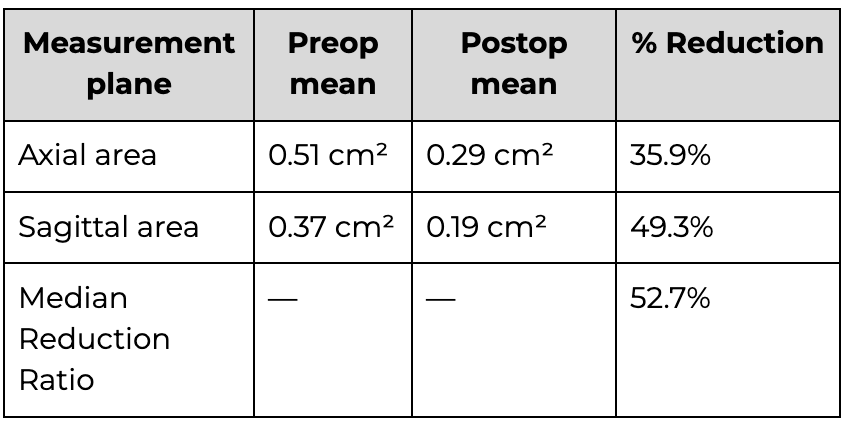
MRI analysis demonstrated a statistically significant reduction in herniated disc size after PLDD:
Clinical outcomes: pain relief and patient satisfaction
In parallel with anatomical improvement, patients experienced remarkable symptom relief:
- Pain scores (NRS) dropped from 8.5 to 2.0 at 1 and 6 months (P < 0.0001)
- Neuropathic pain (DN4 score) decreased from 5 to 1
- 98% of patients reported at least 50% pain relief
- 79% were satisfied, 16% undecided, and only 5% dissatisfied
- No major or minor complications were reported
Interestingly, longer pain duration was linked to greater disc area reduction, a finding attributed to possible biochemical softening or pre-existing degeneration of the disc, making it more responsive to laser decompression.
How PLDD is performed
- Patient lies in the prone position under light sedation
- Local anesthetic is injected at the entry site
- Under X-ray guidance, a spinal needle is inserted into the disc
- Discography is performed to assess integrity
- A laser fiber (400 µm) is advanced through the needle
- Laser energy (7 joules per burst) is delivered in pulses until 800 joules are reached
- Antibiotic (Gentamycin) is injected into the disc
- Patient is monitored and discharged the same day
Analysis of predictors and outcomes
The study also examined the factors that predicted better outcomes.
Key findings:
- Pain duration positively correlated with:
- Greater sagittal area reduction (P = 0.04)
- Higher overall reduction ratio (P = 0.008)
- No correlation found with:
- Age
- Gender
- Body Mass Index (BMI)
- Surgical level
This suggests that long-standing disc pathology may be more responsive to laser decompression, potentially due to chronic dehydration or structural weakening of disc tissue.
The science behind PLDD: how laser energy helps
The mechanism of PLDD is based on closed hydraulic system theory. By vaporizing a small portion of the nucleus pulposus, the laser:
- Reduces intradiscal pressure
- Relieves mechanical nerve root compression
- Potentially limits inflammatory responses triggered by annular strain
Research confirms that even a 10% volume reduction in the nucleus can lead to substantial pressure drops within the disc space.
Comparison with other treatments
Conservative therapy:
- NSAIDs, corticosteroids, and physical therapy
- Works in ~80% of cases
- Delayed relief, risk of recurrence
Microdiscectomy:
- Gold standard for extruded discs
- Involves bone and ligament removal
- Higher complication rate (5–10%)
- Requires general anesthesia
PLDD:
- Minimally invasive, no general anesthesia
- Effective for contained herniations
- Faster recovery, no hospitalization
- No major adverse events in the study
Limitations of the study
While findings are encouraging, the study has certain limitations:
- Small sample size (58 patients)
- No control group for conservative therapy comparison
- Short-term follow-up (2 months MRI, 6 months clinical)
- Single observer for MRI measurements (no inter-rater reliability test)
Future research should include randomized controlled trials, longer follow-up periods, and possibly evaluate PLDD in combination with disc regenerative therapies.
Conclusion
PLDD is a compelling option for patients who:
- Have a contained disc herniation
- Experience persistent pain despite 4+ months of conservative treatment
- Are not ideal candidates for open surgery
- Prefer a less invasive approach with faster recovery
It is not a cure-all but fills a crucial gap between conservative care and invasive surgery. With careful patient selection, PLDD offers:
- Measurable reduction in herniated disc size
- Consistent pain relief
- High satisfaction and safety profile
Recommendations for clinical practice
- Assess disc type via MRI before offering PLDD
- Avoid PLDD in patients with sequestered discs or prior surgeries
- Use PLDD as bridge therapy before committing to open surgery
- Follow up with post-op MRI at 2 months for monitoring
For more information, refer to the full article in Pain Medicine.
Gazzeri R, Occhigrossi F, Galarza M, Mercieri M, Leoni MLG. Radiological analysis of herniated disc size changes after percutaneous laser disc decompression. Pain Med. 2025;26(11):741-748.
For a detailed case study on PLDD and more, download NYSORA’s Pain Medicine Assistant App!