
Regional anesthesia is increasingly recognized as an essential component of pediatric anesthetic care. Its benefits are clear: reduced postoperative pain, decreased opioid consumption, and faster recovery, all of which improve outcomes and minimize adverse events. However, most anatomical knowledge underpinning pediatric regional anesthesia is extrapolated from adult studies. Neonates and infants are not simply “small adults”—their anatomy differs in ways that may significantly affect the accuracy and safety of nerve blocks.
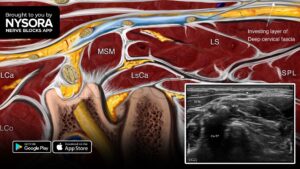
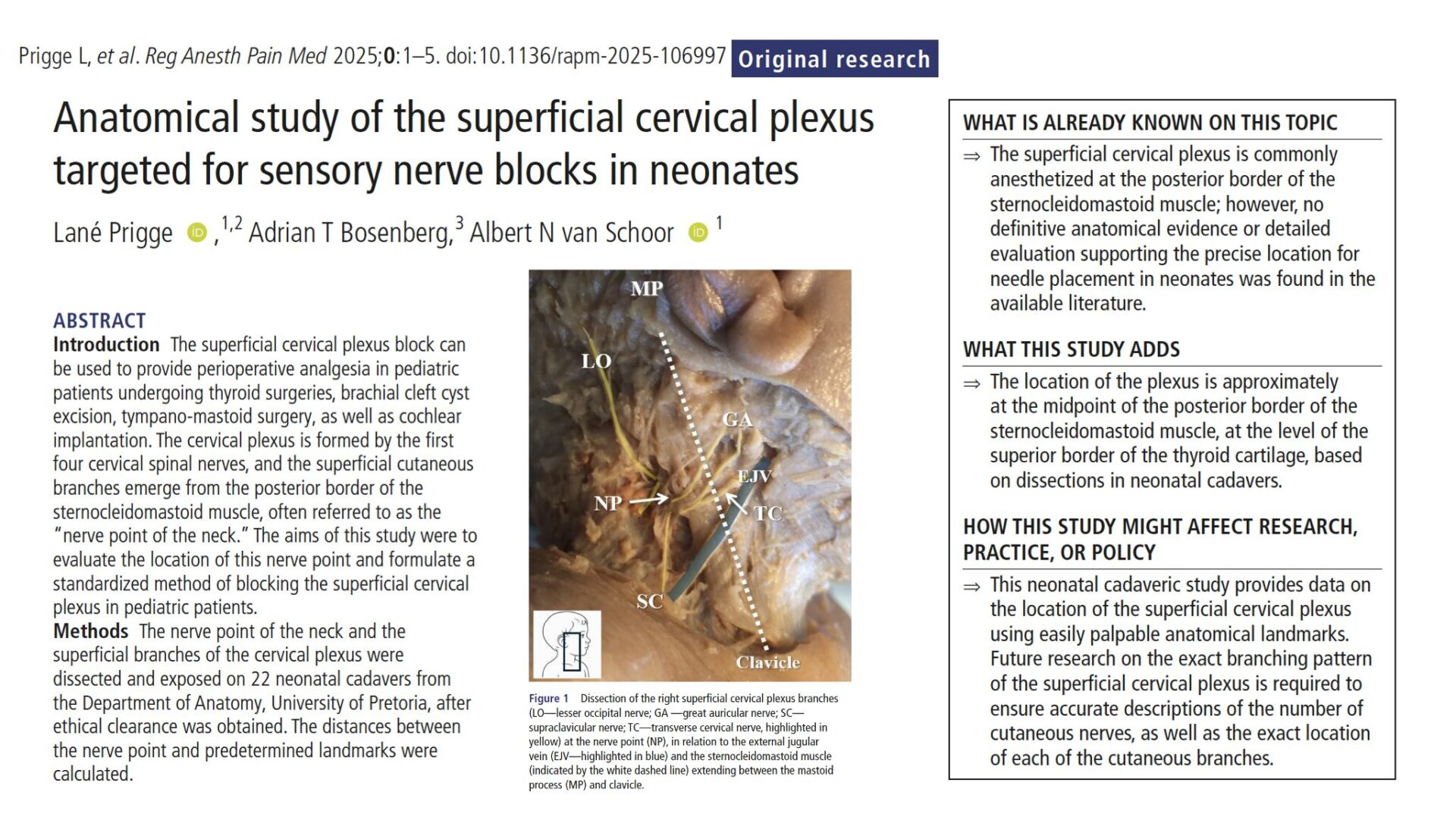
The superficial cervical plexus (SCP), formed by the anterior rami of C1–C4, provides sensory innervation to the anterolateral neck and areas of the head and shoulder. Its cutaneous branches (great auricular, lesser occipital, supraclavicular, and transverse cervical nerves) typically emerge at the midpoint of the posterior border of the sternocleidomastoid (SCM)—a landmark often called the “nerve point of the neck.” In adults, this nerve point is a reliable target for SCP blocks, widely applied for thyroidectomy, mastoidectomy, cleft excision, and cochlear implantation.
Until now, little anatomical data existed for neonates, leaving clinicians to rely on adult-derived assumptions. This study by Prigge et al. aimed to define neonatal-specific anatomy of the SCP, providing evidence-based landmarks for safe and effective nerve blocks in the youngest patients.
Study objective and methods
The primary objective of this anatomical study was to precisely locate the superficial cervical plexus in neonates and establish standardized anatomical landmarks to guide SCP blocks.
-
- Design: Observational, cross-sectional anatomical study.
- Setting: Department of Anatomy, University of Pretoria, South Africa.
- Subjects: 22 embalmed neonatal cadavers (0–28 days old, normal birth weight, no congenital abnormalities).
- Dissection protocol:
-
- Supine positioning with contralateral head rotation to simulate patient positioning.
- Layered dissection of the cervical region to expose the SCP at its emergence from the posterior border of the SCM.
- Identification of cutaneous branches (great auricular, lesser occipital, supraclavicular, and transverse cervical nerves).
- Relation to the external jugular vein (EJV) was noted.
- Measurements:
-
- Distance from nerve point (NP) to SCM attachments (mastoid and clavicle).
- NP distance to EJV and midline of the neck.
- Correspondence of NP to the thyroid cartilage level.
Key findings
- The nerve point of the neck in neonates was located 17.5 mm from the mastoid attachment and 19.8 mm from the clavicular attachment of the SCM.
- On average, it lay ~ 21 mm lateral to the midline of the neck.
- In 83% of cases, the nerve point aligned with the superior border of the thyroid cartilage, providing a consistent clinical landmark.
- The nerve point was positioned ~ 4.7 mm posterior to the external jugular vein, underscoring the need for caution during landmark-based infiltration.
- The superficial branches consistently emerged along the posterior border of the SCM, though slightly more cranially than in adults.
- Both intra- and inter-rater reliability were excellent (ICC > 0.98), confirming high reproducibility of measurements.
Conclusion
This cadaveric study delivers the first neonatal-specific anatomical mapping of the superficial cervical plexus. Unlike in adults, where the nerve point is classically described at the SCM midpoint, in neonates it lies slightly more cranially but reliably at the level of the superior thyroid cartilage and just posterior to the EJV. These findings support a refined, pediatric-specific landmark approach for superficial cervical plexus blocks, improving both safety and accuracy in neonatal regional anesthesia.
Future research
- Branching patterns: The study did not document individual cutaneous nerve trajectories—future studies should map these for selective nerve targeting.
- Depth measurements: Skin-to-nerve distances were not assessed due to dissection limitations; ultrasound studies could address this.
- Ultrasound correlation: Integrating anatomical data with imaging validation in live infants is essential for clinical translation.
- Older infants and children: Anatomy likely changes with growth—longitudinal studies are needed.
- Clinical outcomes: Prospective trials should confirm whether these landmarks improve block success, safety, and analgesic outcomes in pediatric surgery.
Clinical implications
By demonstrating that the nerve point is most consistently found at the level of the superior border of the thyroid cartilage and posterior to the EJV, the results establish reliable palpation-based guides that differ from adult anatomy. These findings caution against simply extrapolating adult references to children and highlight the need for pediatric-specific approaches. Clinically, the use of precise landmarking allows for smaller local anesthetic volumes, reducing the risk of systemic toxicity and enhancing safety in neonates. Moreover, the identification of consistent, easily located landmarks has educational value, providing a simplified framework for teaching trainees and standardizing practice in pediatric regional anesthesia.
Clinical pearls
- Nerve point ≈ 21 mm lateral to midline at thyroid cartilage level.
- Slightly cranial relative to adult “mid-SCM” descriptions.
- EJV lies ≈ 4.7 mm anterior—mind intravascular risk.
- 83% alignment with superior thyroid cartilage provides a dependable level.
- High measurement reliability supports clinical translation.
Practical tip: Target the midpoint of the posterior SCM at the thyroid cartilage level for accurate neonatal SCP blocks.
For more detailed information, refer to the full article in RAPM.
Prigge L. et al. Anatomical study of the superficial cervical plexus targeted for sensory nerve blocks in neonates. Reg Anesth Pain Med. Published online August 27, 2025.
Download the Nerve Blocks App HERE for in-depth insights on 60+ nerve block techniques from head to toe. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Manual Module on NYSORA360!