This chapter will probably be the shortest. It was necessary to understand quietly, step-by-step, the elementary sign, the developed sign of interstitial syndrome, and the phenomenon of lung sliding. Lung ultrasound is a dynamic tool investigating a dynamic organ, using a sign, lung sliding, with no equivalent using traditional tools (X-rays and CT mainly). This allows to define two opposing kinds of interstitial syndrome, the transudative and the exudative interstitial syndrome.
In the BLUE-protocol, they were given short labels:
- The detection in a blue patient, at the anterior chest wall, of lung rockets associated with lung sliding (each word is important) has been called the B-profile
- The B’-profile is a B-profile with abolished lung sliding
This distinction follows the logic of the BLUE-protocol, by determining profiles using associations of signs [1]. When we write that lung sliding is “abolished” in the B’-profile, it can be completely, or quite completely abolished, with a 1-mm amplitude roughly. This distinction is of no relevance: both cases indicate a very impaired compliance. The question of pneumothorax makes no sense in the presence of any B-line. Note interestingly that videos are not mandatory if good quality M-mode data are provided.
The B-profile and mostly the B’-profile are seen independently from the type of ventilation (spontaneous or mechanical).
1. THE ULTRASOUND TRANSUDATIVE INTERSTITIAL SYNDROME (B-PROFILE)
Briefly, hemodynamic pulmonary edema generates transudate, a kind of oil preventing the lung to burn during an all-life breathing. Usually, the B-profile will be seen in hemodynamic pulmonary edema.
2. THE ULTRASOUND EXUDATIVE INTERSTITIAL SYNDROME (B’-PROFILE)
Inflammatory diseases generate exudate, fibrin, and various viscous stuffs, which may stick the lung to the wall. The B’-profile will prove a highly specific sign of pneumonia/ARDS. (Fig. 1)
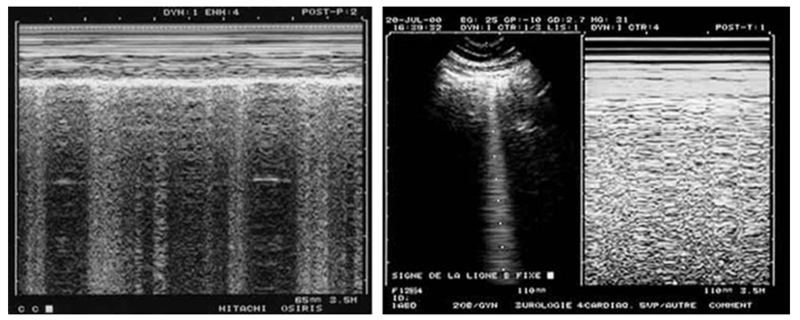
Fig. 1 This figure is devoted to show that static images can indicate dynamic phenomena. To the left, the alternation of vertical hyperechoic lines shows that B-lines come and go through the shooting line of the M-mode: lung sliding is present. Note also the marked dyspnea in the Keye’s space: patient likely not intubated. To the right, the M-mode shows a homogeneous field below the Keye’s space, indicating that the B-line taken by the shooting line is standstill.
3. THE LANGUAGE OF THE BLUE-PROTOCOL, ITS MAIN PRINCIPLE
The label “B-profile” should be understood, like in aviation language, where speed is life, and where most pieces of information must be said in a minimal time. Instead of “B-profile,” one could have said: “the pattern with ten features, which is a comet-tail artifact, arising from the pleural line, moving with lung sliding, usually long, usually well-defined, usually erasing A-lines, usually hyperechoic, multiple (three or more) in one longitudinal scan, disseminated to the anterior bilateral chest wall, and moving with a preserved lung sliding,” a little long for being adopted. Words are the principle of any language. In usual conditions, the “B-profile” and the “B’-profile” are recognized in a few seconds or less. One of the immediate therapeutic outcomes is the suggestion of CPAP in the case of a B-profile and direct intubation in the case of a B’-profile, as seen in the detailed chapters.