Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About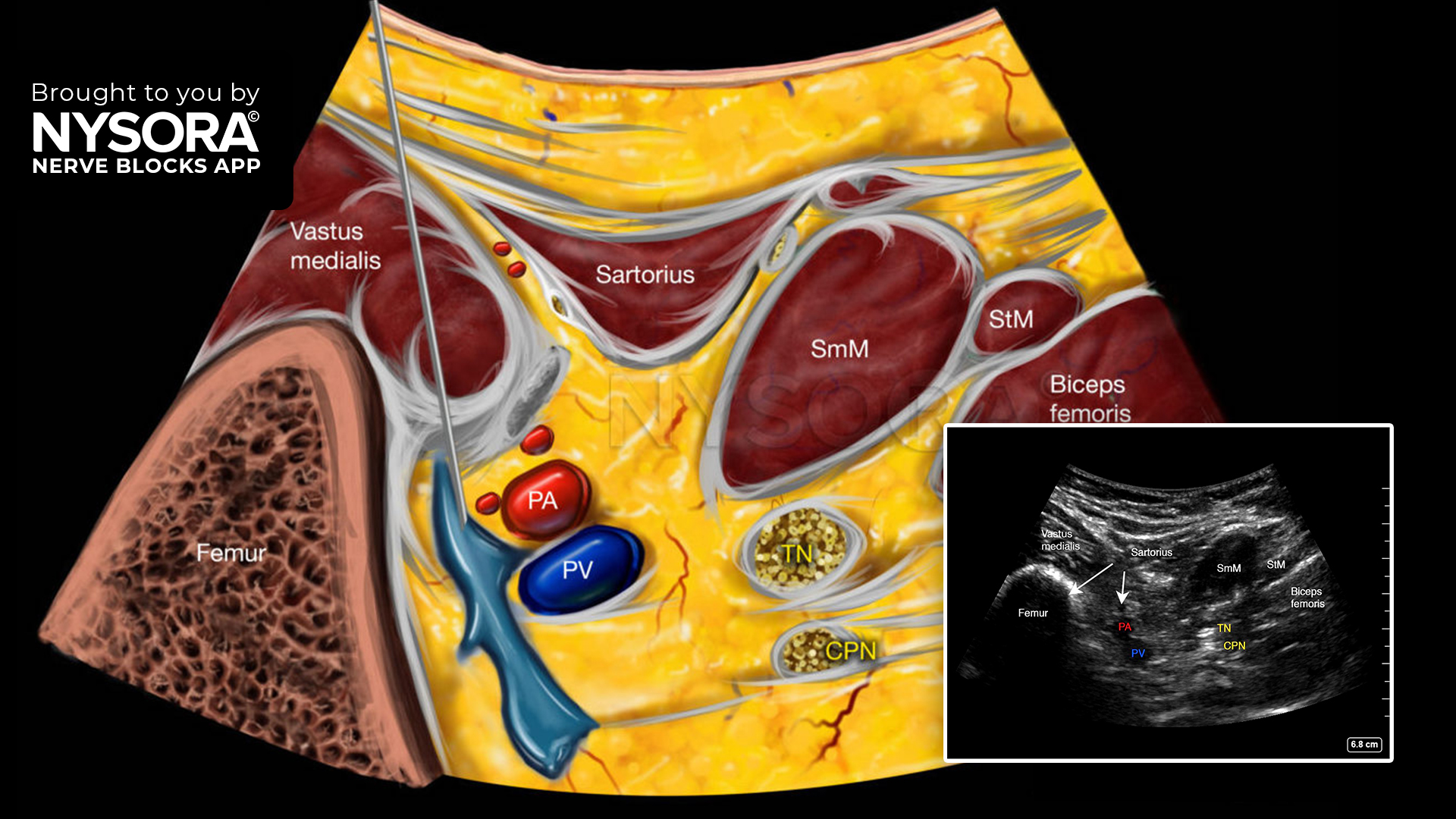
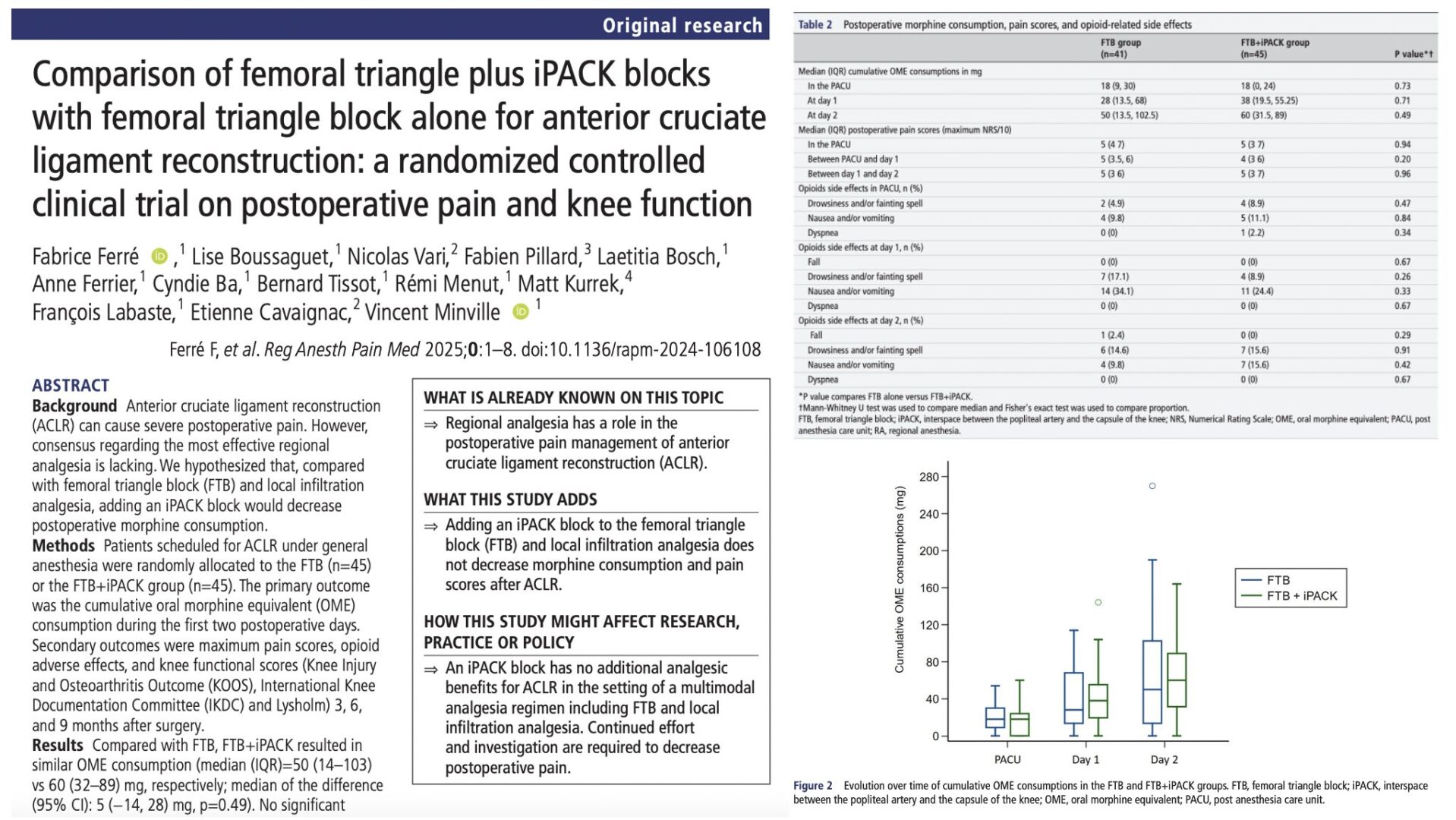
In recent years, advancements in regional anesthesia have significantly improved post-operative pain management for anterior cruciate ligament (ACL) reconstruction. One of the most promising techniques is the iPACK (infiltration between the popliteal artery and capsule of the knee) block. This innovative, motor-sparing block is gaining attention for its ability to target posterior knee pain while preserving motor function, an essential factor for early rehabilitation. A randomized controlled trial, led by Martin and colleagues, compared the efficacy of combining the femoral triangle block with the iPACK block against traditional local infiltration analgesia in ACL reconstruction patients.
Understanding the iPACK Block
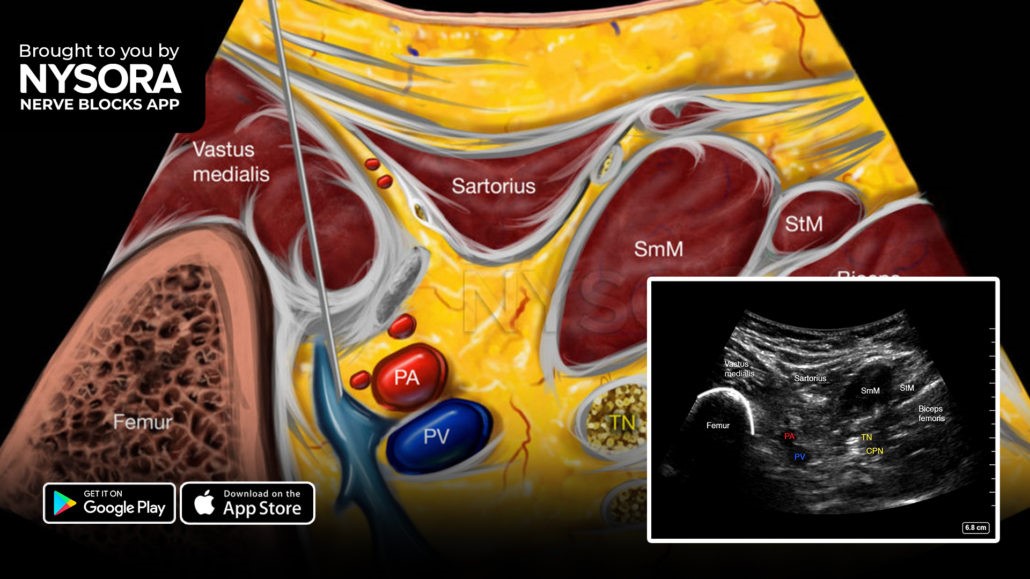
The IPACK block, designed as a motor-sparing technique, involves the injection of local anesthetic into the space between the popliteal artery and the posterior capsule of the knee. It offers a supplementary pain management solution to the femoral nerve or adductor canal blocks, specifically for posterior knee pain. By targeting the sensory articular branches of the sciatic nerve and avoiding the motor branches of the tibial and common peroneal nerves, the IPACK block circumvents the motor weakness and foot drop associated with traditional sciatic nerve blocks, facilitating early rehabilitation without masking potential intraoperative injuries to the common peroneal nerve.
Methods
- 60 patients undergoing ACL reconstruction were divided into two groups:
- One group received a combination of femoral triangle block and iPACK
- The other group received traditional local infiltration analgesia.
- Both groups were administered a total of 160 mg of ropivacaine, and post-operative pain was managed with patient-controlled intravenous morphine, acetaminophen, and ibuprofen.
- The primary outcome was the total morphine consumption within the first 24 hours post-surgery.
- Secondary outcomes included pain scores at 2 and 24 hours and functional measures such as range of motion and quadriceps strength at various intervals post-surgery.
Key Findings
- The study found that the combination of femoral triangle block and iPACK significantly reduced morphine consumption at 24 hours compared to the local infiltration analgesia group (9.7 mg vs. 17.0 mg, p=0.03).
- Notably, the two groups had similar pain-related and functional outcomes, including pain scores and muscle strength.
Why the iPACK Block is Important
- Motor-Sparing Advantage: By targeting only sensory nerves, the iPACK block avoids motor nerve involvement, preventing muscle weakness and allowing early mobility. This is crucial for patients undergoing ACL reconstruction, where early mobilization and physical therapy are essential for recovery.
- Opioid-Sparing Benefits: With the opioid crisis posing a significant public health challenge, reducing the need for post-operative opioids is a top priority. The iPACK block, when combined with the femoral triangle block, substantially lowers morphine consumption without sacrificing pain relief, presenting a safer, more sustainable approach to post-operative care.
- Targeted Posterior Pain Relief: Traditional nerve blocks, such as the femoral or adductor canal blocks, are effective for anterior and lateral knee pain but often fall short of addressing posterior discomfort. The iPACK block fills this gap by providing localized analgesia to the posterior knee, improving overall pain management.
Conclusion
The iPACK block represents a significant advancement in post-operative pain management for ACL reconstruction. Its ability to spare motor function while effectively controlling posterior knee pain makes it an ideal complement to other regional anesthesia techniques. By combining femoral triangle block and iPACK, clinicians can provide a complete pain management solution, minimizing the need for opioids and facilitating early rehabilitation—a win for both patients and healthcare providers.
For more detailed information, refer to the full article in Regional Anesthesia and Pain Medicine.
Martin R, Kirkham KR, Ngo THN, Gonvers E, Lambert J, Albrecht E. Combination of femoral triangle block and infiltration between the popliteal artery and the capsule of the posterior knee (iPACK) versus local infiltration analgesia for analgesia after anterior cruciate ligament reconstruction: a randomized controlled triple-blinded trial. Reg Anesth Pain Med. 2021;46(9):763-768.
Follow these 3 key steps for a successful IPACK block
- Place the transducer transversely over the medial aspect of the knee, 2-3 cm above the patella.
- Slide the transducer proximal and distal to identify the distal femoral shaft and popliteal artery.
- Insert the needle in-plane, from the anteromedial aspect of the knee, toward the space between the popliteal artery and femur, and inject 15-20 mL of local anesthetic.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App in book format – the perfect study companion with the Nerve Blocks app!