
Tips for a Supraclavicular Brachial Plexus Block
The supraclavicular approach blocks the brachial plexus from the distal trunks to the proximal cords or at the level of the brachial plexus divisions. This block is used for analgesia in upper extremity surgeries. The block was first introduced in 1911 by Kulenkampff as a landmark-based approach and popularized by Dr. Alon Winnie in the 1970s. Kapral and colleagues re-invented the block using ultrasound to decrease the risk of pneumothorax and intravascular injection. The technique is very reliable, and also known as the “spinal anesthesia of the upper extremities.”
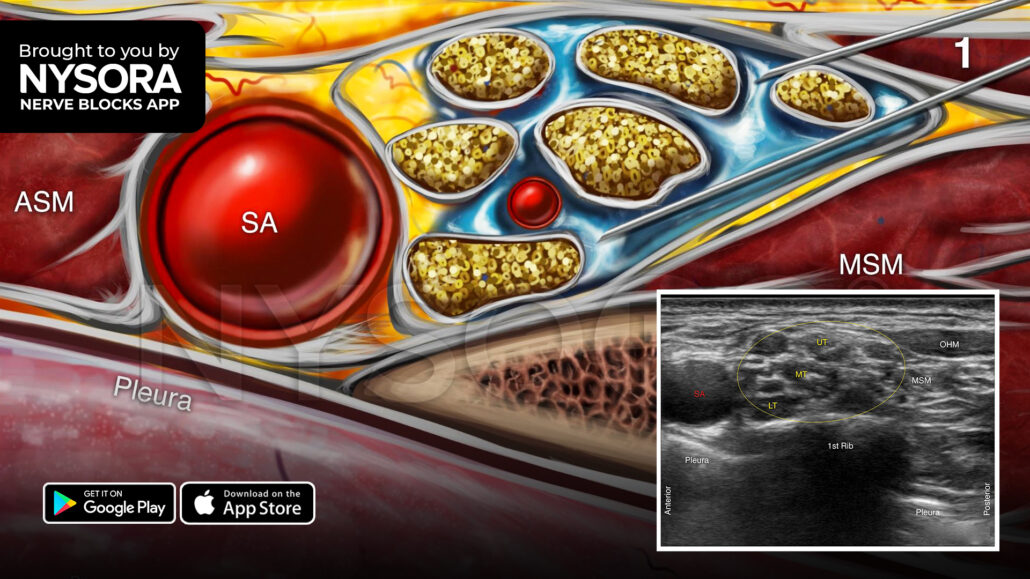
Here are 3 tips to successfully perform a supraclavicular brachial plexus block
- The initial insertion of the needle should not be deeper than 1 cm since the brachial plexus is shallow at this location.
- Visualize the needle path at all times to reduce the risk of pneumothorax.
- The neck is highly vascular, so use the color Doppler to detect any large vessels (i.e., dorsal scapular artery, transverse cervical artery, suprascapular artery) in the needle path.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!











