Several alternative analgesic techniques have been recently suggested for hip pain (e.g., surgery, fractures, chronic pain). They all consist of an injection of a local anesthetic in proximity to the acetabulum, and in the plane between the iliopsoas muscle and the proximal insertion of the anterior hip capsule. The techniques vary in the transducer orientation, needle insertion and recommended volumes of local anesthetic. This new addition to NYSORA’s web-app is the approach used in our clinical practice for patients who qualify for fast-track after a primary total hip replacement (anterior approach).
Functional Anatomy
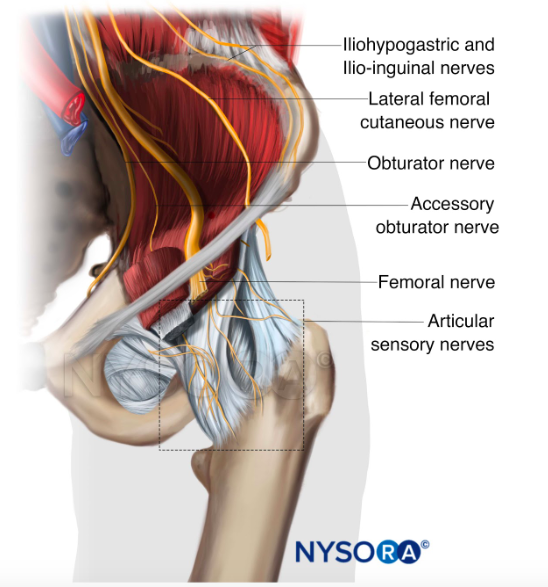
Pain after total hip replacement comes primarily from the anterior hip capsule which is innervated by the terminal nerves of the lumbar plexus:
- Femoral nerve: The articular branches from the femoral nerve reach the plane between the iliopsoas muscle and the iliofemoral ligament (iliopsoas plane) and innervate the anterior and lateral aspects of the hip capsule.
- Obturator nerve: The articular branches innervate the anterior and medial aspects of the hip capsule.
- Accessory obturator nerve: Contributes to the innervation of the hip in 10%-30% of the patients, and supplies the inferomedial aspect of the hip capsule.
The cutaneous innervation of the anterolateral thigh is conferred by the lateral femoral cutaneous nerve (LFCN), which travels underneath the inguinal ligament, medially to the anterior superior iliac spine (ASIS) and courses distally, superficial to the sartorius muscle.
The posterior aspect of the hip joint is innervated by the sciatic nerve and branches of the sacral plexus (superior and inferior gluteal nerves, and an articular branch from the quadratus femoris nerve).