
Ultrasound-Guided Ankle Block: NYSORA Web App
Here’s how to perform an ankle block, one of the most useful regional anesthesia techniques for foot surgery. Among its advantages, the preservation of ankle mobility facilitates unassisted ambulation allowing faster recovery after surgery. Ultrasound guidance allows for precise identification of each nerve and superficial branches together with a consistent block using lower volumes of local anesthetic.
Technique description
The ankle block involves anesthetizing two deep nerves (tibial and deep peroneal) and three superficial cutaneous nerves (superficial peroneal, sural and saphenous nerve).
We routinely block the deep nerves first and then the superficial cutaneous ones. The saphenous nerve block is usually not necessary for surgeries on the forefoot and toes. In most patients, the saphenous nerve does not reach the toes.
To block the tibial nerve
- Place the transducer transversely between the medial malleolus and the Achilles tendon (Fig-1).
- Identify the tibial nerve as an oval hyperechoic structure next to the posterior tibial artery and veins, deep to the flexor retinaculum.
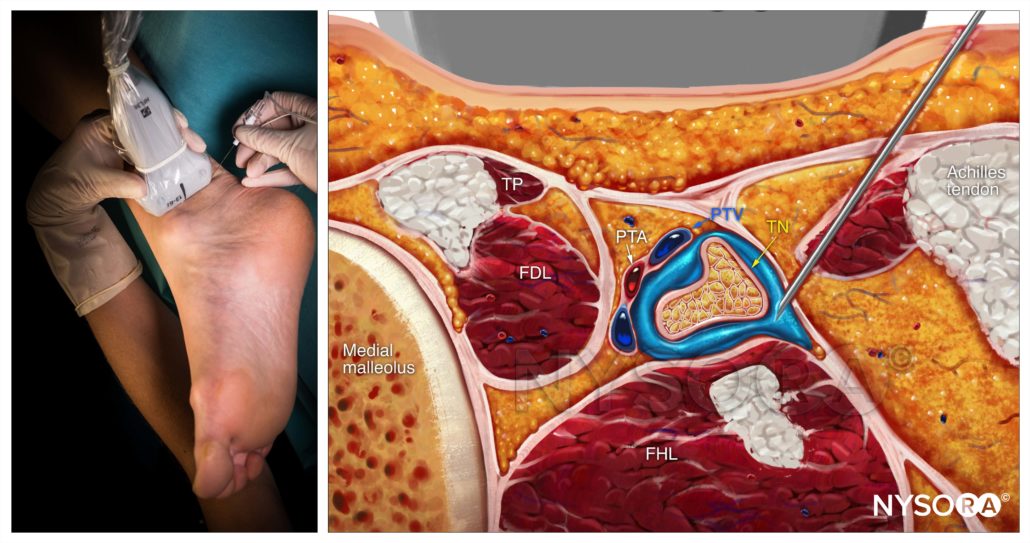
- Insert the needle using an in-plane or out-of-plane approach toward the fascia enveloping the nerve (Fig-2).
- Inject 1-2 mL to confirm proper needle position by observing local anesthetic spread into the fascial plane containing the nerve and surrounding the nerve.
- Complete the block with a volume of 5-8 mL
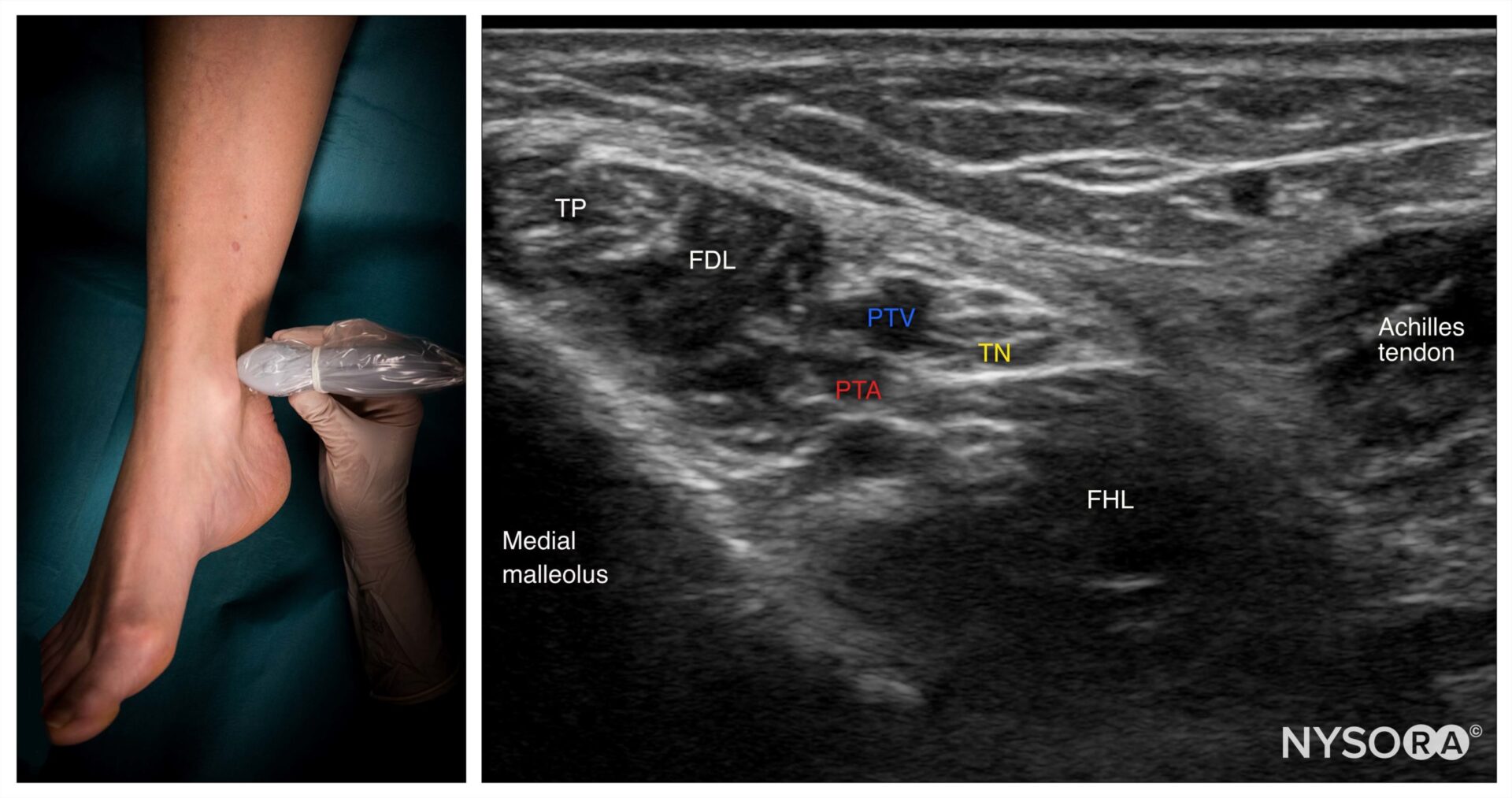 Fig-1. Transducer position and sonoanatomy for a tibial nerve block. TP, Tibialis posterior muscle; FDL, Flexor digitorum longus; PTA, Posterior tibial artery; PTV, posterior tibial vein; TN, Tibial nerve; FHL, Flexor hallucis longus.
Fig-1. Transducer position and sonoanatomy for a tibial nerve block. TP, Tibialis posterior muscle; FDL, Flexor digitorum longus; PTA, Posterior tibial artery; PTV, posterior tibial vein; TN, Tibial nerve; FHL, Flexor hallucis longus.
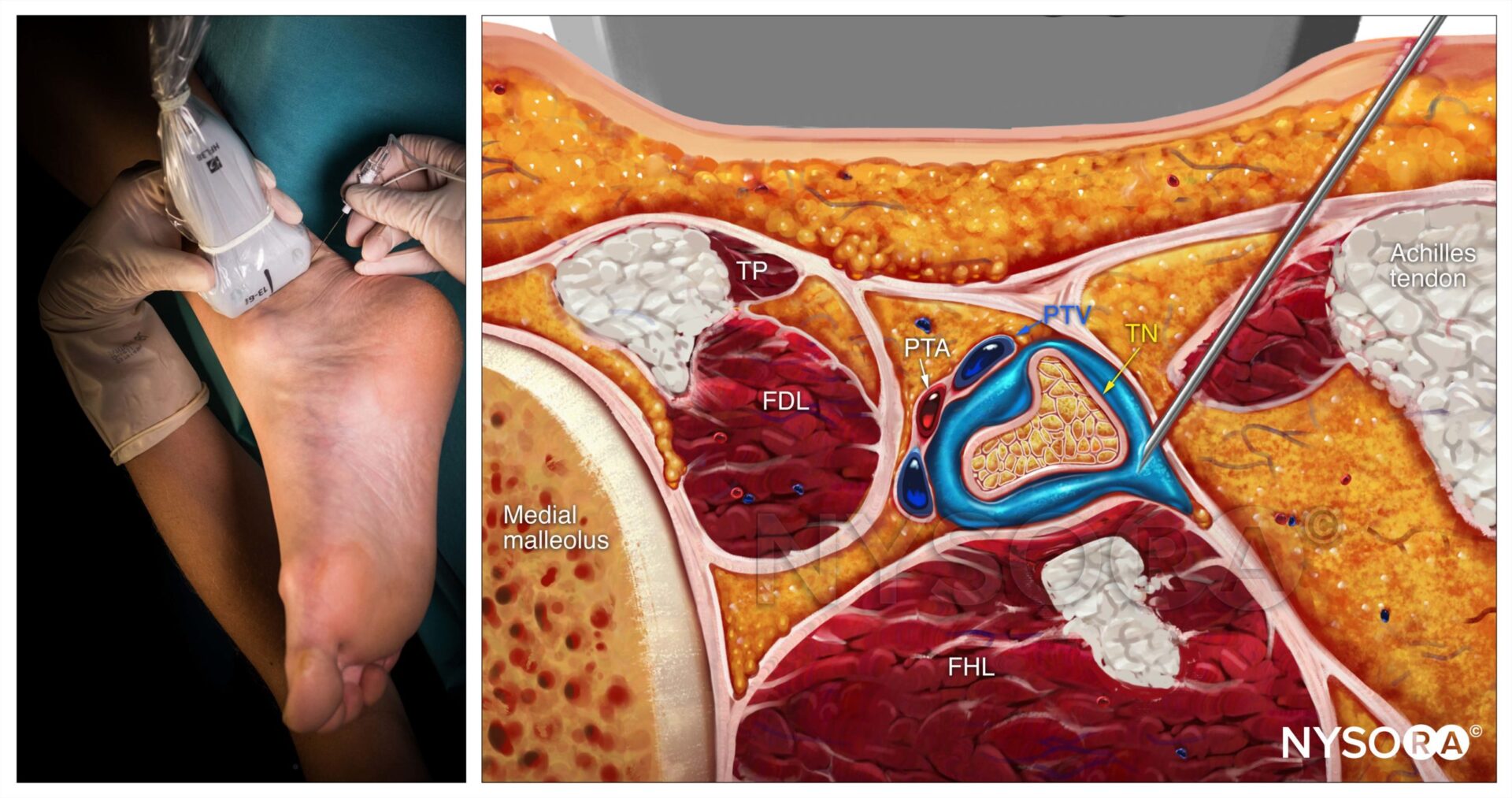 Fig-2. Reverse ultrasound anatomy of a tibial nerve block with needle insertion in-plane. TP, tibialis posterior muscle; FDL, flexor digitorum longus; PTA, posterior tibial artery; PTV, posterior tibial vein; TN, tibial nerve; FHL, flexor hallucis longus.
Fig-2. Reverse ultrasound anatomy of a tibial nerve block with needle insertion in-plane. TP, tibialis posterior muscle; FDL, flexor digitorum longus; PTA, posterior tibial artery; PTV, posterior tibial vein; TN, tibial nerve; FHL, flexor hallucis longus.
To block the deep peroneal nerve
- Place the transducer in a transverse orientation on the anterior aspect of the ankle (Fig-3).
- Identify the nerve as two small hypoechoic nodules with a hyperechoic rim lateral or superficial to the anterior tibial artery over the surface of the tibia.
- Insert the needle using an in-plane or out-of-plane approach (Fig-4).
- Inject 1-2 mL to confirm proper needle position by observing spread within the fascial plane displacing the nerve away from the needle.
- Complete the block with a volume of 3-5 mL of local anesthetic next to the nerve.
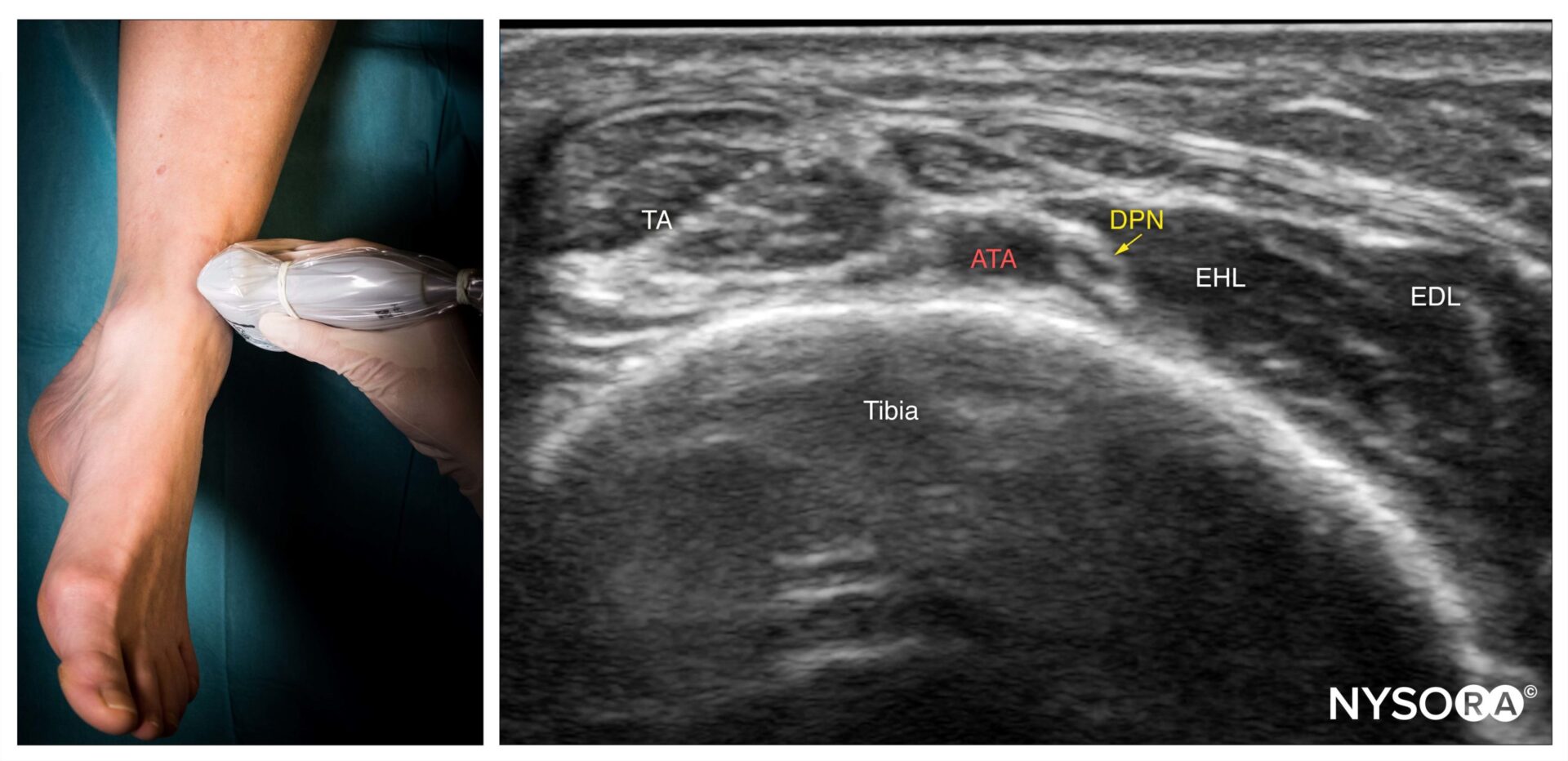 Fig-3. Transducer position and ultrasound anatomy of the deep peroneal nerve. TA, tibialis anterior muscle; ATA, anterior tibial artery; DPN, deep peroneal nerve; EHL, extensor hallucis longus; EDL, extensor digitorum longus.
Fig-3. Transducer position and ultrasound anatomy of the deep peroneal nerve. TA, tibialis anterior muscle; ATA, anterior tibial artery; DPN, deep peroneal nerve; EHL, extensor hallucis longus; EDL, extensor digitorum longus.
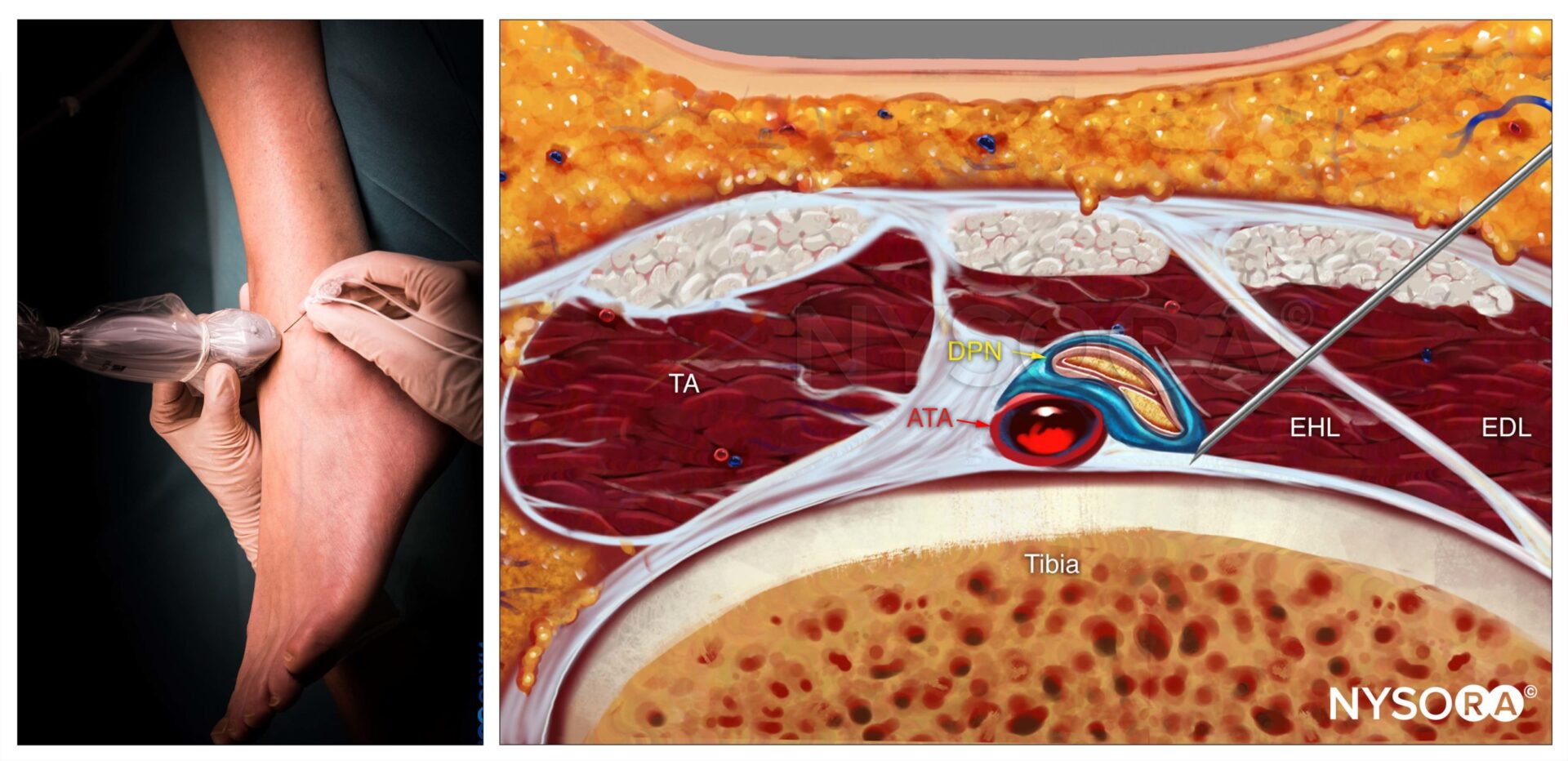 Fig-4. Reverse ultrasound anatomy of a deep peroneal nerve block with needle insertion in-plane. TA, tibialis anterior muscle; ATA, anterior tibial artery; DPN, deep peroneal nerve; EHL, extensor hallucis longus; EDL, extensor digitorum longus.
Fig-4. Reverse ultrasound anatomy of a deep peroneal nerve block with needle insertion in-plane. TA, tibialis anterior muscle; ATA, anterior tibial artery; DPN, deep peroneal nerve; EHL, extensor hallucis longus; EDL, extensor digitorum longus.
To learn more about the ankle block and gain access to continuous educational updates, subscribe to the NYSORA Web App.










