
- Learn
-
Apps
View all apps
Veterinary
 VetRA App
VetRA App

- Books
- Events
- News
- Partners
- About
- For Clinicians
 VetRA App
VetRA App
Rapid bedside diagnosis app for the heart, lungs, abdomen, vascular access, and more. Master your emergency diagnostics skills on the go!


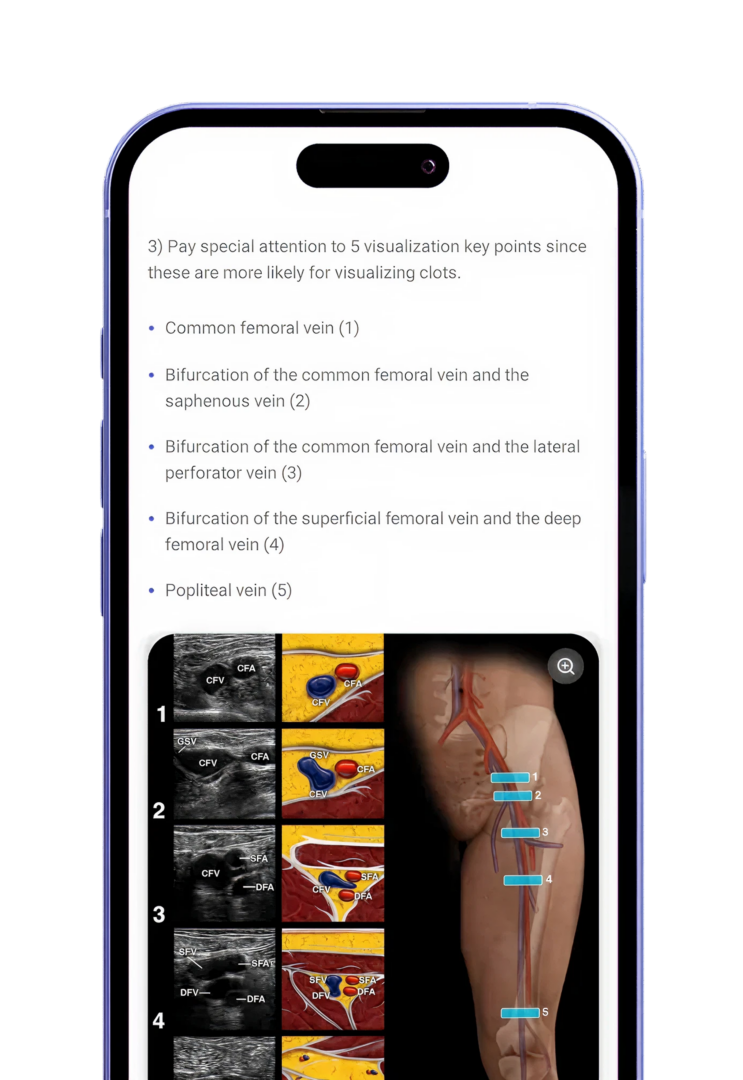
Vascular, lung, abdominal, and more.
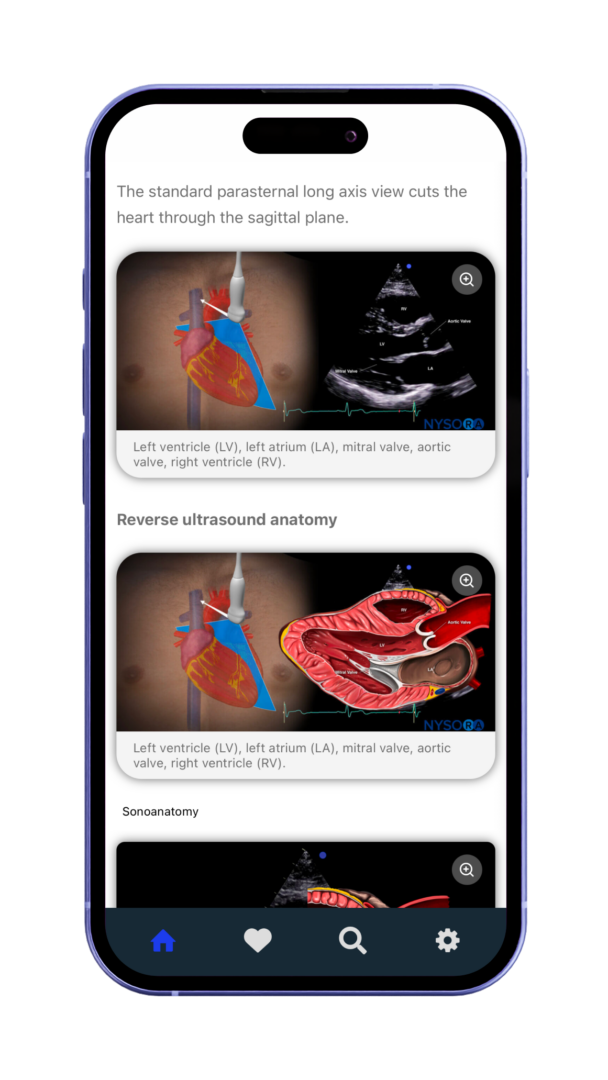
Reverse Ultrasound Anatomy illustrations make sonoanatomy easier to understand and apply.
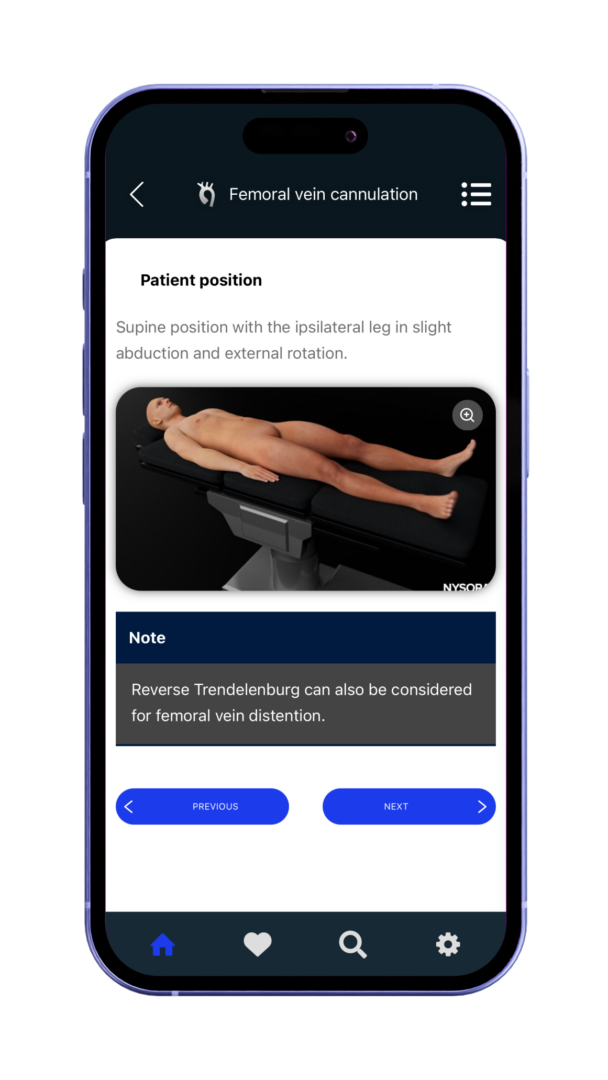
Optimized for fast, easy access on mobile and tablet devices in clinical practice.
Vascular, lung, abdominal, and more.
Reverse Ultrasound Anatomy illustrations make sonoanatomy easier to understand and apply.
Optimized for fast, easy access on mobile and tablet devices in clinical practice.
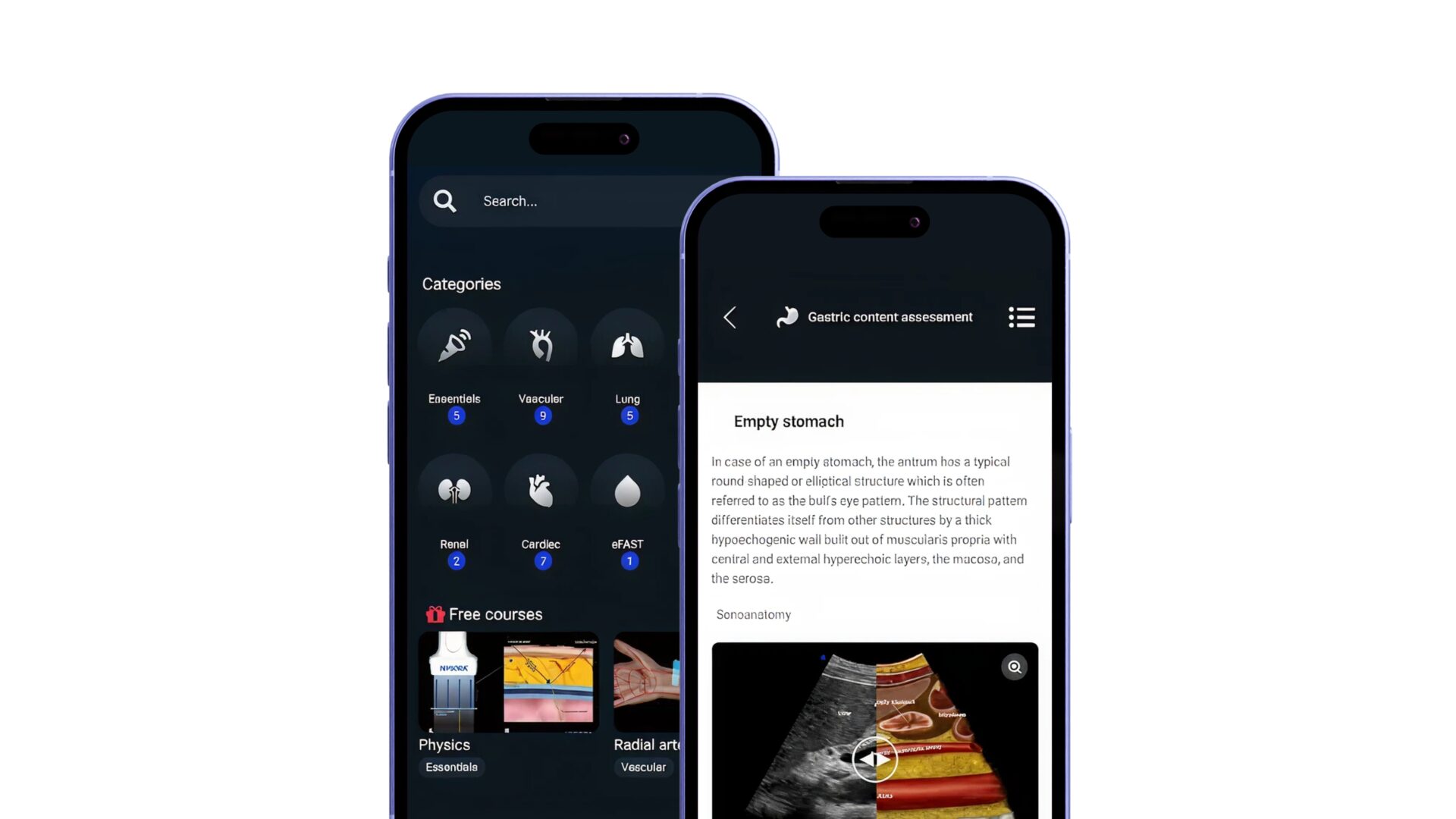
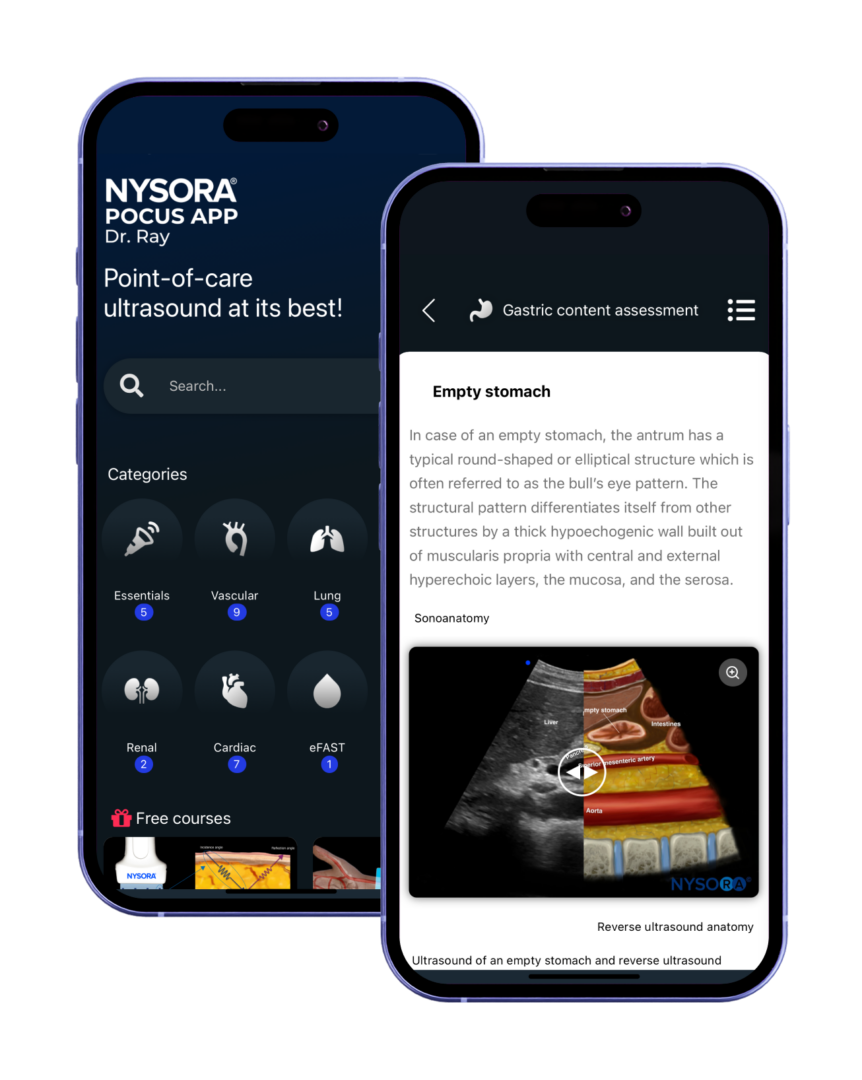
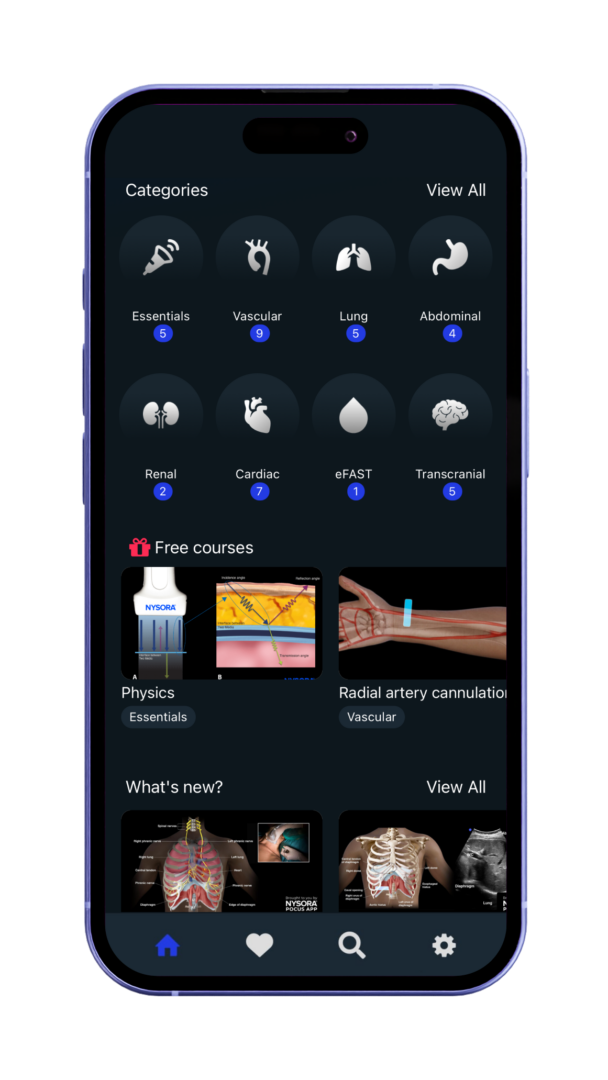
The best mobile guide for point-of-care-ultrasound. Trusted by physicians worldwide.




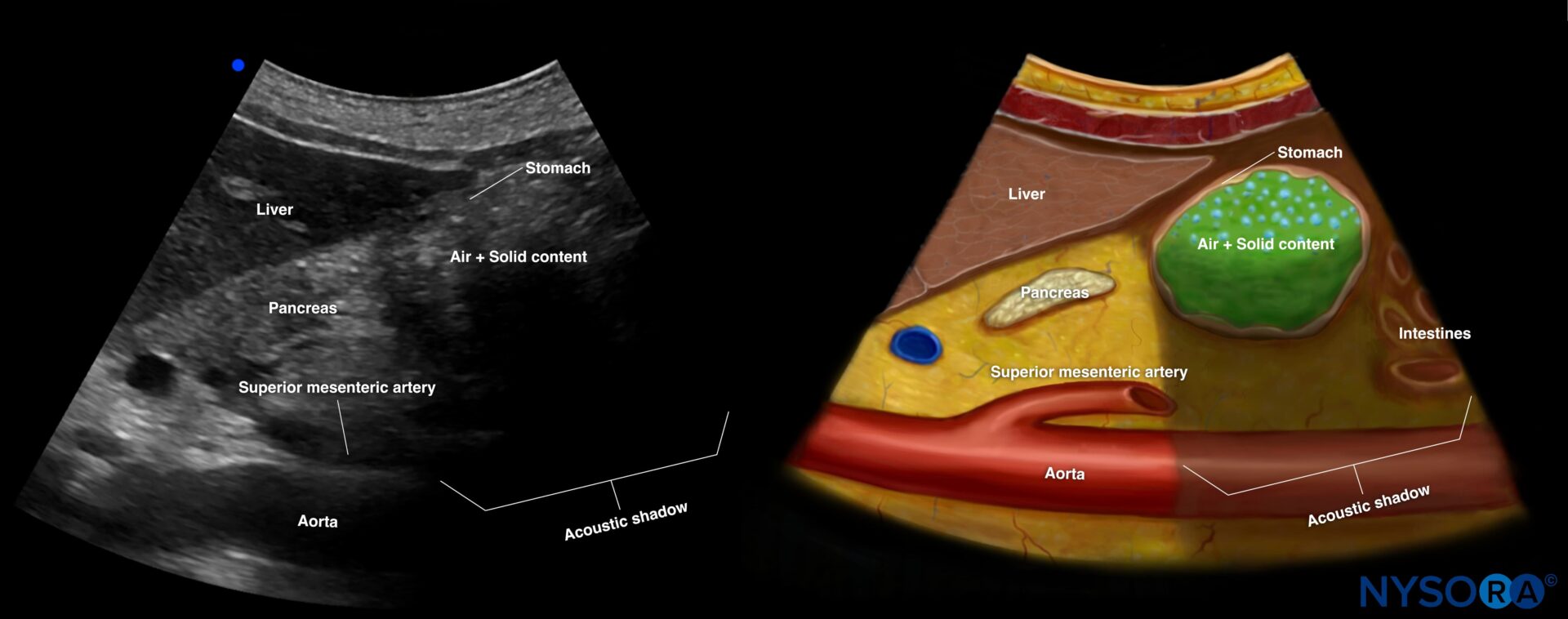
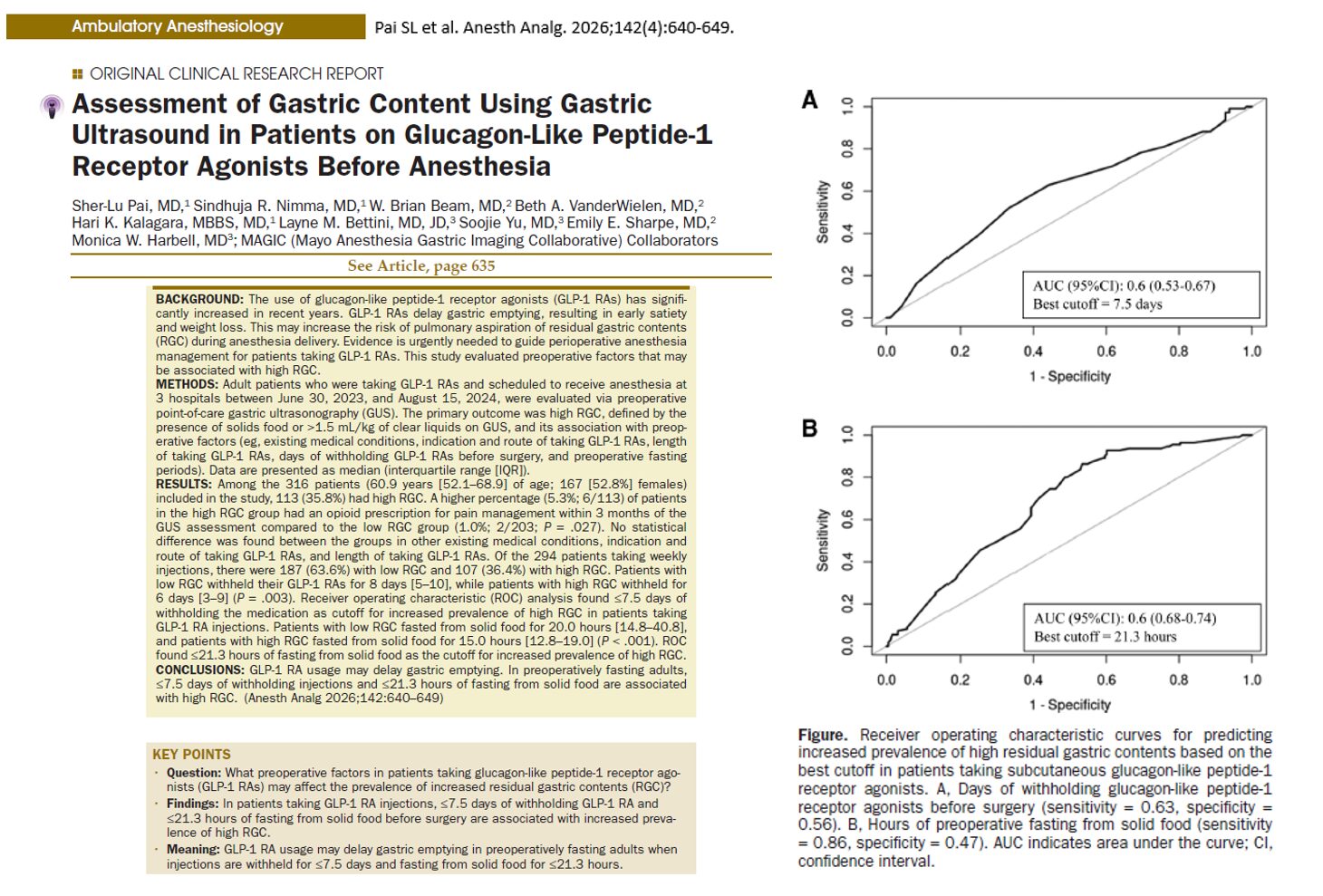
Introduction The widespread adoption of glucagon-like peptide-1 receptor agonists (GLP-1 RAs), such as semaglutide and tirzepatide, has transformed the management of type 2 diabetes mellitus and obesity. However, emerging evidence is raising important concerns for anesthesiologists and perioperative clinicians. A new clinical study from the Mayo Clinic, published in Anesthesia & Analgesia (2026), provides critical insights into how these medications influence gastric physiology and potentially increase the risk of pulmonary aspiration during anesthesia. What are GLP-1 receptor agonists? GLP-1 receptor agonists are incretin-based therapies that: Enhance glucose-dependent insulin secretion Suppress glucagon release Slow gastric emptying Promote satiety and weight loss Common medications include: Semaglutide Tirzepatide Dulaglutide Liraglutide Their ability to delay gastric emptying is central to both their therapeutic benefits and perioperative risks. Why delayed gastric emptying matters in anesthesia Pulmonary aspiration occurs when gastric contents enter the lungs during anesthesia, potentially leading to: Aspiration pneumonitis Acute respiratory distress syndrome (ARDS) Increased perioperative morbidity and mortality Standard fasting guidelines (e.g., 6–8 hours for solids) aim to minimize this risk. However, GLP-1 RAs may disrupt this safety margin. Study overview Design and population 316 adult patients on GLP-1 RAs Conducted across three Mayo Clinic centers Preoperative evaluation using gastric ultrasound (GUS) Definition of high-risk gastric content Solid food present Or >1.5 mL/kg of gastric fluid volume Key findings High prevalence of residual gastric contents 35.8% of patients had high residual gastric content (RGC) This occurred despite adherence to fasting guidelines Insufficient medication withholding increases risk Patients with high RGC withheld GLP-1 RAs for a shorter duration Critical cutoff: ≤7.5 days before surgery increased risk Fasting duration is crucial Patients with high RGC fasted for shorter periods Critical cutoff: ≤21.3 hours for solid food This is significantly longer than standard fasting recommendations. Opioid use may worsen gastric retention Higher prevalence of recent […]
Introduction Pulmonary aspiration remains one of the most feared complications in obstetric anesthesia. Although rare, it carries significant maternal and neonatal morbidity. A comprehensive 2026 review published in the European Journal of Anaesthesiology provides updated insights into gastric physiology during pregnancy, labor, and the postpartum period, along with the evolving role of gastric ultrasound. Anatomy and physiology of the stomach The stomach is a distensible muscular organ divided into four main regions: Cardia Fundus Body Pylorus Its primary physiological roles include: Temporary storage of food and fluids Mechanical and chemical digestion Regulation of gastric emptying into the duodenum Secretion of intrinsic factor Modulation of appetite and satiety Key physiological insight Basal gastric acid secretion and acidity do not change during pregnancy What causes pulmonary aspiration? For aspiration to occur, three conditions must be met: Presence of sufficient gastric contents Reduced lower oesophageal sphincter (LOS) tone Suppressed airway reflexes Pregnancy-specific changes LOS pressure decreases progressively, reaching a nadir at ~36 weeks Intragastric pressure increases due to the gravid uterus Risk increases significantly under general anesthesia Gastric emptying during pregnancy First trimester Gastric emptying of liquids is delayed Likely influenced by hormonal changes and early pregnancy physiology Second and third trimesters No significant difference in gastric emptying for: Liquids Solids Clinical takeaway Early pregnancy poses a higher risk of delayed gastric emptying than later stages Gastric emptying during labor Labor significantly alters gastric physiology. Without analgesia or opioids Gastric emptying is delayed for both liquids and solids With systemic opioids Further slowing of gastric emptying With epidural analgesia Gastric emptying improves However, it does not return to nonpregnant levels Postpartum gastric physiology Gastric emptying returns to nonpregnant baseline levels No significant differences observed within the first 5 days postpartum Gastric ultrasound: a game-changing tool Gastric ultrasound has become a critical bedside tool […]




The best mobile guide for point-of-care-ultrasound. Trusted by physicians worldwide.
The app includes:
The NYSORA POCUS App provides quick access to expertly-curated content, helping you:
The app covers:
The app can be used in multiple ways:
It’s a mobile-friendly reference tool offering:
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About