Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About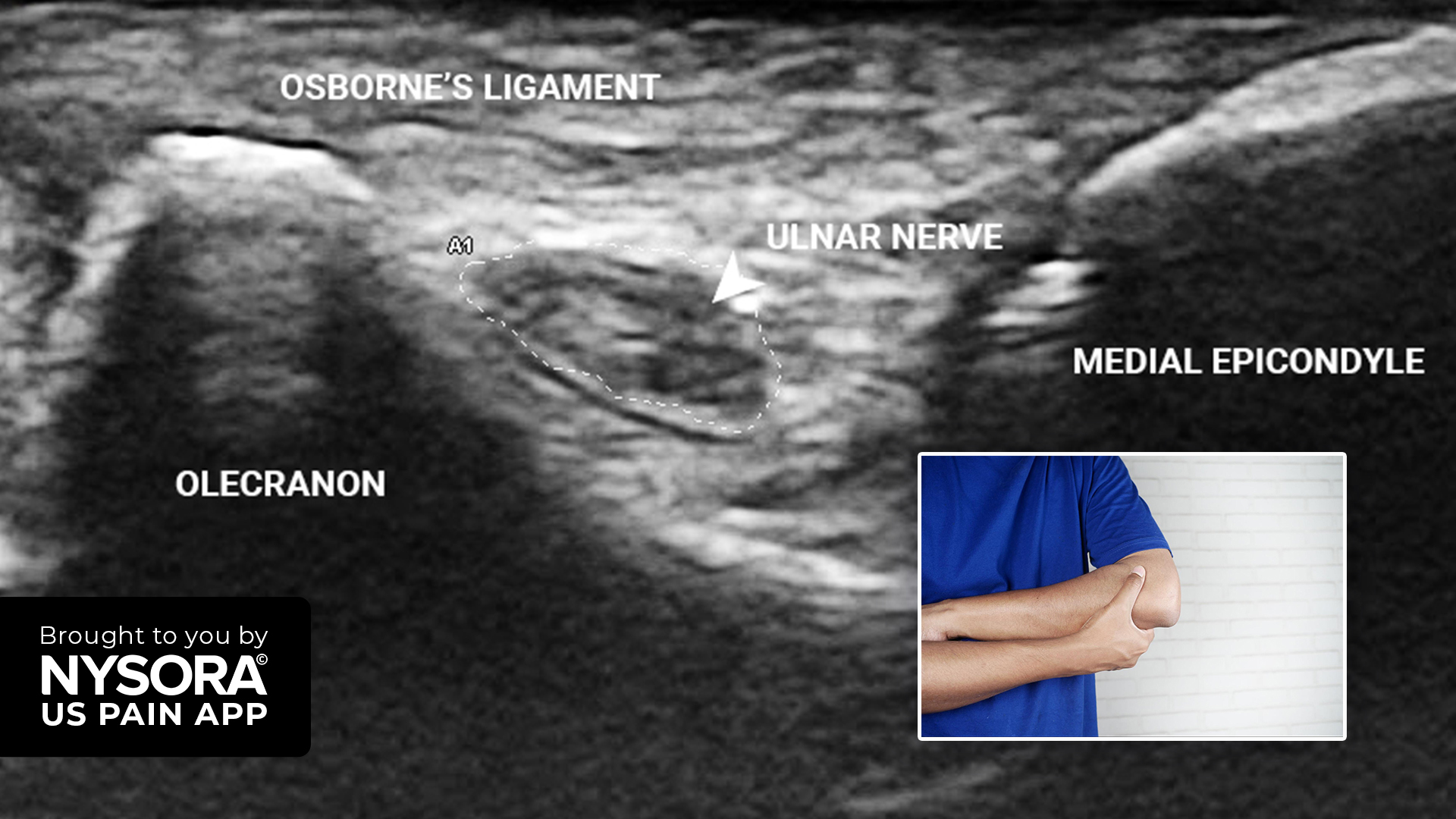

A 65-year-old orthopedic surgeon presents with pain along the ulnar aspect of the right forearm and hand, lasting for one year. The patient does not report any weakness in these areas and has no comorbidities. He previously underwent an ulnar nerve hydrodissection, a procedure to relieve pressure around the nerve, which reduced the pain by 80%. However, due to persistent occasional pain along the ulnar border of the forearm, he presented for further treatment.
Physical examination
- Pain was not associated with any activity and there were no relieving factors
- No redness or wasting of the forearm
- No hypothenar wasting
- No evidence of ulnar claw hand
- Tinel sign: Positive
- Sensation: Light touch and 2-point discrimination were normal Froment’s sign: Negative
Ultrasound findings
MRI imaging revealed an ulnar nerve entrapment at the level of the medial epicondyle. The reference value for a swollen nerve is set at ≥ 10 mm2, according to the meta-analysis by Chang et al. (2018).
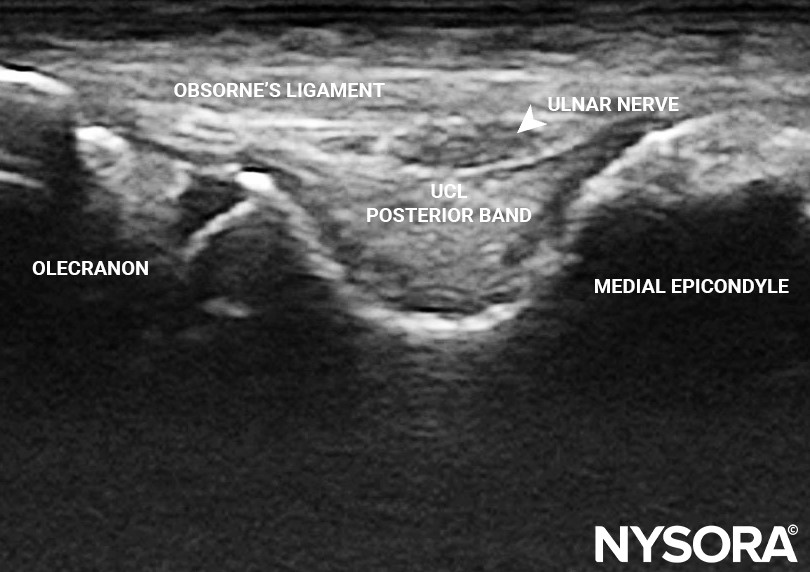
Transverse view of the elbow in a neutral position at the level of the edial epicondyle. Here, the ulnar nerve measured 5.9 x 1.6 mm. UCL, ulnar collateral ligament. m

Transverse view of the elbow in a flexed position at the level of the medial epicondyle. Here, the ulnar nerve measured 3.1 x 6.8 mm.
Diagnosis
The patient was diagnosed with cubital tunnel syndrome, which is caused by the compression of the ulnar nerve at the elbow. The ulnar nerve entrapment leads to numbness and pain in the forearm and specific fingers. It is the second most common neuropathy of the arm after carpal tunnel syndrome.
Discover more about the treatment strategy, patient outcome, and other unique case studies in the US Pain App. Ready to expand your knowledge? Click HERE and get the ultimate app for chronic pain procedures.