



Low back pain (LBP) remains one of the leading causes of disability worldwide, often resulting in reduced quality of life and impaired mobility. For patients with lumbar spinal arthritis, pain related to facet joints can make simple activities like walking increasingly difficult. A new prospective study published in Regional Anesthesia & Pain Medicine delivers encouraging results: radiofrequency ablation (RFA) not only alleviates pain but also improves walking speed, providing a functional, objective measure of success.
This study is the first to directly assess gait velocity as a primary outcome after RFA in patients with facet-mediated LBP, using validated gait analysis technology. It supports the idea that functional mobility, not just subjective pain scores, should be central to how clinicians evaluate treatment effectiveness.
What is radiofrequency ablation?
Radiofrequency ablation is a minimally invasive procedure that uses thermal energy to disrupt the medial branch nerves transmitting pain from the lumbar facet joints. Performed under fluoroscopic guidance, RFA has become a mainstay in treating chronic facet joint pain, especially when patients fail to respond to conservative care such as:
- Physical therapy
- Oral medications (e.g., NSAIDs)
- Lifestyle modifications
Study overview
Conducted at the University of Arkansas for Medical Sciences, this single-center study aimed to go beyond traditional patient-reported outcomes by quantifying functional improvements after RFA.
Inclusion criteria
- Adults over 18 years old
- Chronic low back pain >6 months
- Pain rated >5/10 on a visual analog scale
- Failed conservative management (PT, NSAIDs)
- 80% relief from dual medial branch blocks (MBBs), confirming facet joint pain
Exclusion criteria
- Radicular pain or neurologic symptoms
- Prior lumbar hardware between L3–S1
- Coagulopathies, pregnancy, ASA class >3
- Non-English speakers, those unable to walk 50 feet unaided
Gait analysis: the Zeno Walkway
A central innovation in this study was the use of the Zeno Walkway, a 20×4 foot pressure-sensitive mat widely used in gait research for conditions like Parkinson’s disease. The system offers precise measurements of:
- Velocity (cm/s)
- Stride length and width
- Variability coefficients
Patients were instructed to:
- Stand from a seated position
- Walk the length of the mat
- Turn 180° around a cone
- Return to the start
- Complete three trials per visit (pre- and 4 weeks post-RFA)
Key results
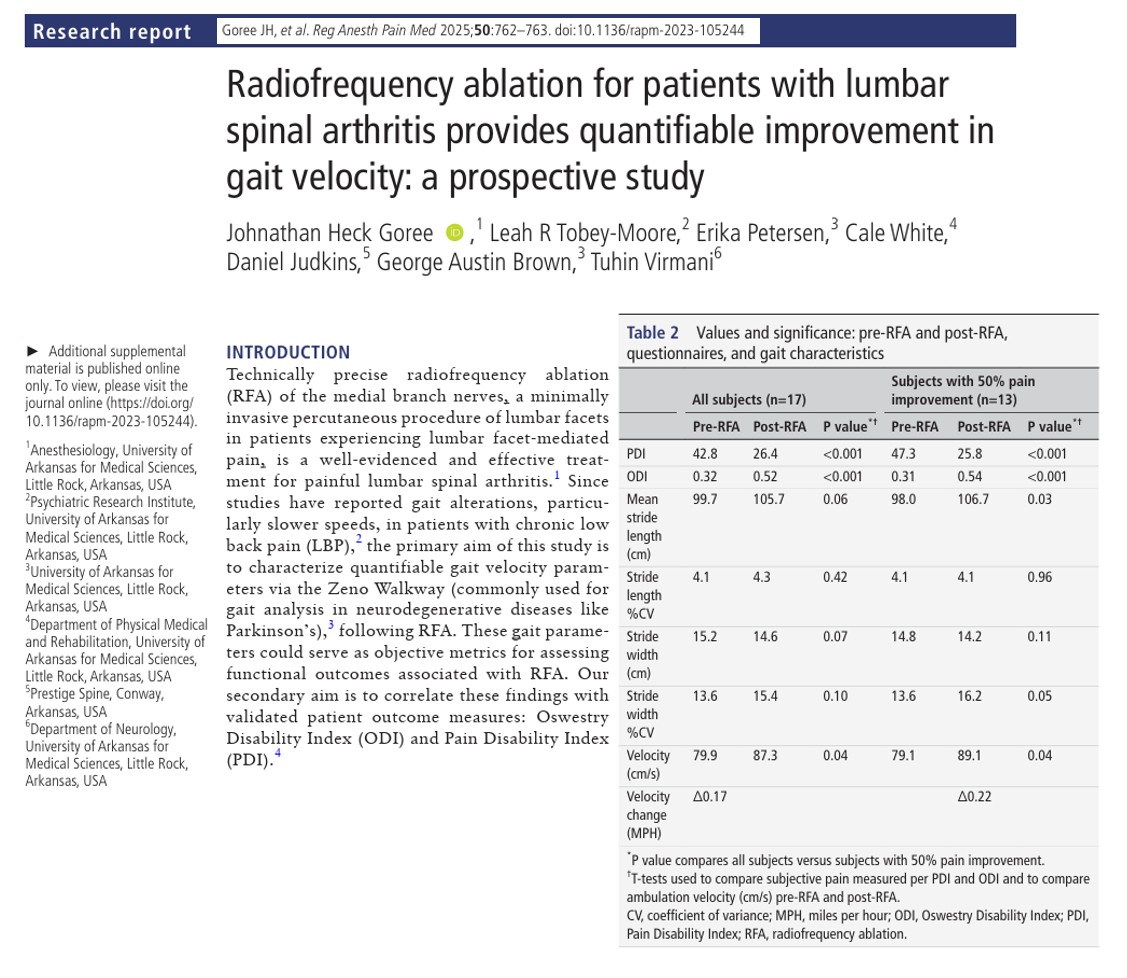
1. Gait velocity improved significantly
- Pre-RFA: 79.9 cm/s (~1.78 mph)
- Post-RFA: 87.3 cm/s (~1.95 mph)
- Velocity change: +0.17 mph overall; +0.22 mph in patients with >50% pain reduction
Why it matters:
Gait velocity improvements of just 0.04–0.06 m/s have been shown to reflect a clinically meaningful reduction in disability or mobility limitation.
2. Pain and disability decreased
- Pain Disability Index (PDI):
- Pre-RFA: 42.8
- Post-RFA: 26.4 (p < 0.001)
- Oswestry Disability Index (ODI):
- Pre-RFA: 0.32
- Post-RFA: 0.52 (p < 0.001)
These results demonstrate both subjective relief and objective functional gain.
3. Stride metrics stable
- No statistically significant changes in stride length or width
- Suggests improvement in velocity was not due to altered gait mechanics, but likely due to pain relief and increased confidence in movement
Functional impact of gait velocity improvements
In older adults and chronic pain populations, gait velocity is associated with:
- Risk of falls
- Frailty
- Cardiovascular health
- Hospitalization and survival rates
Faster gait often correlates with better functional independence and rehabilitation outcomes.
Clinician perspectives
Rethinking success metrics in RFA
Traditionally, pain scores and satisfaction ratings dominate post-procedure evaluations. This study challenges that paradigm by introducing functional movement data as a valuable clinical endpoint.
When to consider RFA with gait metrics:
- Patients with known lumbar facet joint degeneration and preserved motor strength
- Individuals reporting movement-limiting back pain
- Candidates already undergoing gait therapy or physical rehab
Takeaways for pain specialists:
- Incorporate pre- and post-treatment mobility assessments using tools like TUG (Timed Up and Go) or 10-meter walk test if gait labs are unavailable
- Combine gait metrics with pain scores to justify insurance coverage or continued therapy
- Educate patients about the movement benefits of pain therapy
Limitations and future research
Despite its strengths, the study had some constraints:
- Small sample size (n=17)
- Short follow-up (4 weeks)
- Single institution
- No long-term outcome data or comparison to sham procedures
What’s needed next:
- Multicenter trials with larger sample sizes
- Longitudinal studies to track durability of gait improvements
- Comparative studies vs. conservative care or placebo RFA
Clinical implementation: how to integrate gait into your workflow
Here’s a step-by-step clinical pathway based on this study:
- Identify patients with suspected lumbar facet pain
- Confirm diagnosis with dual MBBs (>80% relief)
- Document baseline mobility (TUG test or gait velocity)
- Perform RFA targeting appropriate medial branches
- Re-assess function at 4–6 weeks post-procedure
- Track progress over time with mobility + pain metrics
Summary
This study represents a critical shift in interventional pain management, one that moves beyond subjective relief toward quantifiable, meaningful recovery.
For pain physicians, anesthesiologists, physiatrists, and rehabilitation experts, RFA now holds not only the promise of reduced pain but also enhanced mobility and independence for patients with lumbar facet arthritis.
As medicine evolves toward outcome-driven care, integrating gait velocity as a routine metric could elevate the standard of spine intervention assessments.
For more information, refer to the full article in Regional Anesthesia & Pain Medicine.
Goree JH, Tobey-Moore LR, Petersen E, et al. Radiofrequency ablation for patients with lumbar spinal arthritis provides quantifiable improvement in gait velocity: a prospective study. Reg Anesth Pain Med. 2025;50(9):762-763.
For more information about acute and chronic pain management, get the Ultrasound-Guided Interventional Pain Procedures Manual on NYSORA 360!