Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About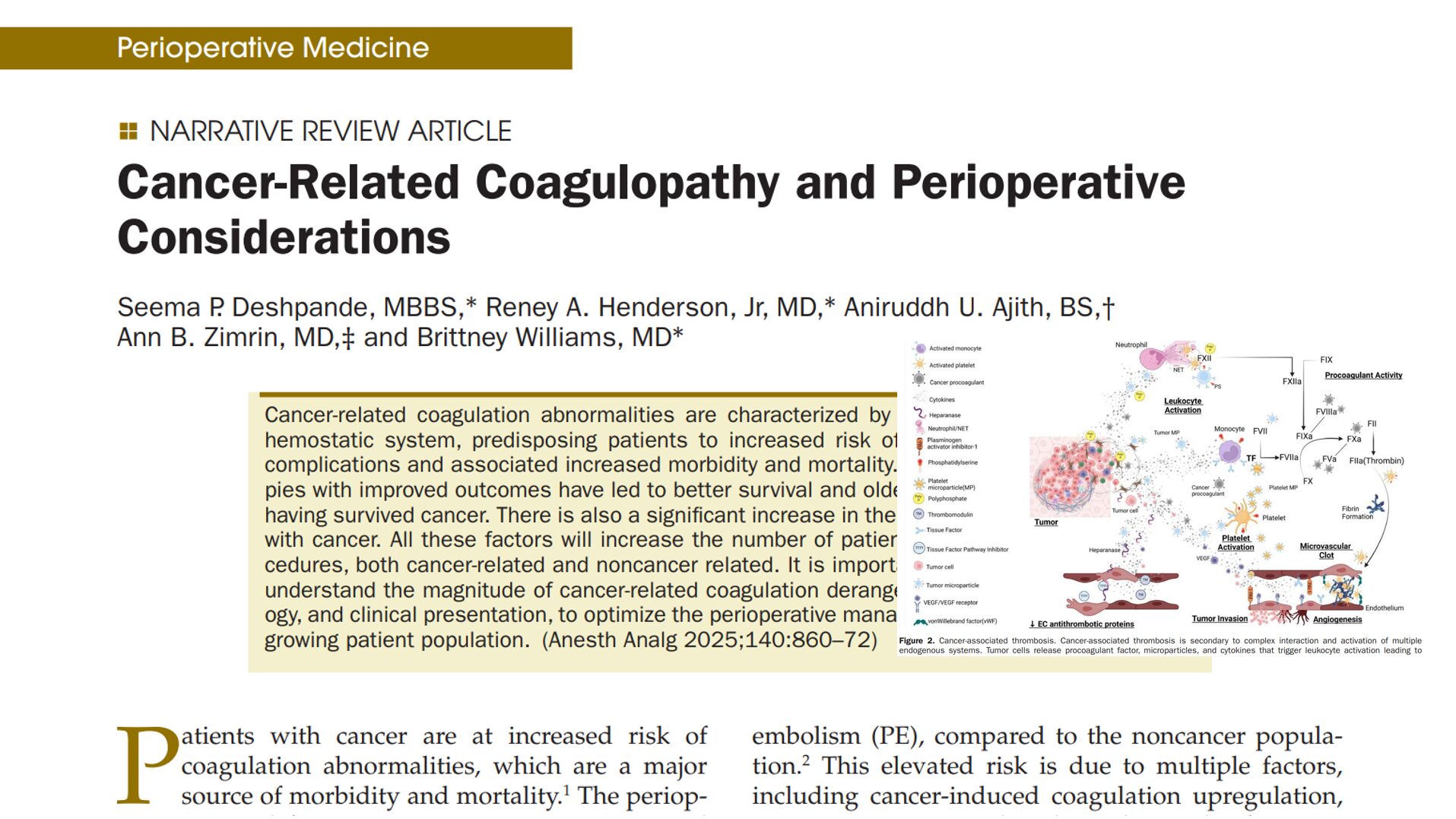



With cancer rates steadily rising and patient survival improving thanks to advanced therapies, anesthesiologists increasingly encounter patients with cancer-related coagulation disorders in the surgical setting. These patients face an elevated risk of both thrombotic and hemorrhagic complications, necessitating a detailed understanding of coagulopathy mechanisms and tailored perioperative strategies.
A review by Deshpande et al. breaks down the complex interplay between malignancy and coagulation.
Epidemiology highlights
- 7–11x increase in venous thromboembolism (VTE) risk in cancer patients.
- 3x higher rate of fatal pulmonary embolism (PE) compared to non-cancer patients.
- Certain malignancies (pancreatic, lung, ovarian) show particularly high VTE risk.
- Hematologic malignancies pose the highest bleeding risk (30% incidence).
- Disseminated intravascular coagulation (DIC) occurs in up to:
- 10% of solid tumors
- 20% of hematologic cancers
Mechanisms
- Tissue Factor (TF) overexpression: Activates the extrinsic coagulation pathway.
- Microparticles (MPs): Released by tumor and blood cells; rich in TF and procoagulant phospholipids.
- Neutrophil Extracellular Traps (NETs): Trigger clot formation and platelet aggregation.
- Hypoxia and HIF-1α activation: Promotes endothelial damage and TF upregulation.
- VEGF overproduction leads to angiogenesis and vascular fragility.
Clinical manifestations
Thrombotic disorders
- VTE: DVT, PE, upper extremity thrombosis (esp. with central lines).
- Arterial thrombosis: Stroke, myocardial infarction; linked to myeloproliferative neoplasms.
- TMA: Hemolytic anemia, thrombocytopenia, renal dysfunction.
- Veno-Occlusive Disease (VOD): Post-transplant liver failure.
- Nonbacterial Thrombotic Endocarditis (NBTE): Valvular vegetations with systemic emboli.
Bleeding disorders
- DIC: Dual presentation of thrombosis and bleeding.
- Thrombocytopenia: Due to chemotherapy, marrow infiltration, or DIC.
- Acquired von Willebrand disease: Especially in hematologic cancers.
- Drug-induced platelet dysfunction: Seen with ibrutinib, anti-VEGF therapies.
Preoperative management
Preoperative evaluation checklist
- Assess cancer type and stage.
- Review treatment history: chemotherapy, radiation, immunotherapies.
- Check coagulation labs:
- Platelet count
- PT/INR, PTT
- D-dimer
- Viscoelastic testing (TEG or ROTEM)
- Evaluate functional status and comorbidities.
Risk stratify with RAMs (Risk Assessment Models):
- Khorana Score
- Caprini RAM (for surgical patients)
- COMPASS-CAT (for ambulatory cancer patients)
Anticoagulation strategy
- Discontinue DOACs (direct oral anticoagulants) 2–3 days before surgery (longer if renal function is impaired).
- Bridging with LMWH (low molecular weight heparin) may be required.
- Avoid regional anesthesia unless coagulation status is corrected per ASRA (American Society of Regional Anesthesia) guidelines.
Intraoperative management
Best practices
- Monitor with TEG/ROTEM to assess clotting efficiency.
- Prepare for:
- Platelet transfusion
- Cryoprecipitate (for low fibrinogen levels)
- Low-dose Prothrombin Complex Concentrates (PCCs)
- Use leukocyte-reduced or irradiated blood products in immunocompromised patients.
Emergencies to watch for
- DIC (Disseminated Intravascular Coagulation): Treat with targeted transfusions, fibrinogen concentrate, and PCCs.
- Acute PE (Pulmonary Embolism) or MI (Myocardial Infarction): Use intraoperative TEE (transesophageal echocardiography); consider ECMO or thrombectomy if indicated.
Postoperative management
Guidelines
- Begin pharmacologic thromboprophylaxis once bleeding is controlled.
- Continue thromboprophylaxis for 4 weeks postoperatively in high-risk patients (e.g., those undergoing major pelvic or abdominal surgeries).
- Combine mechanical and pharmacologic methods when possible.
Duration of VTE prophylaxis
Score 5–8 (Moderate risk):
- Continue VTE prophylaxis for 10 days after surgery.
- These patients have sufficient risk to warrant extended prophylaxis beyond the immediate hospital stay.
Score ≥ 9 (High risk):
- Continue VTE prophylaxis for 30 days postoperatively.
- These patients have significantly elevated risk and benefit from prolonged prevention strategies.

Impact of common chemotherapeutic agents on coagulation and hemostatic risk

Final thoughts
Cancer-associated coagulopathy is multifactorial, dynamic, and highly individualized. With a rapidly evolving therapeutic landscape and aging patient population, perioperative teams—especially anesthesiologists—must remain vigilant and proactive in managing bleeding and thrombotic risks.
Collaborative, evidence-based protocols and real-time assessment tools like ROTEM/TEG are essential to improving outcomes in this vulnerable population.
For more information on this topic, check out Anesthesia Updates on the NYSORA Anesthesia Assistant App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.