
Explore NYSORA knowledge base for free:
Explore NYSORA knowledge base for free:
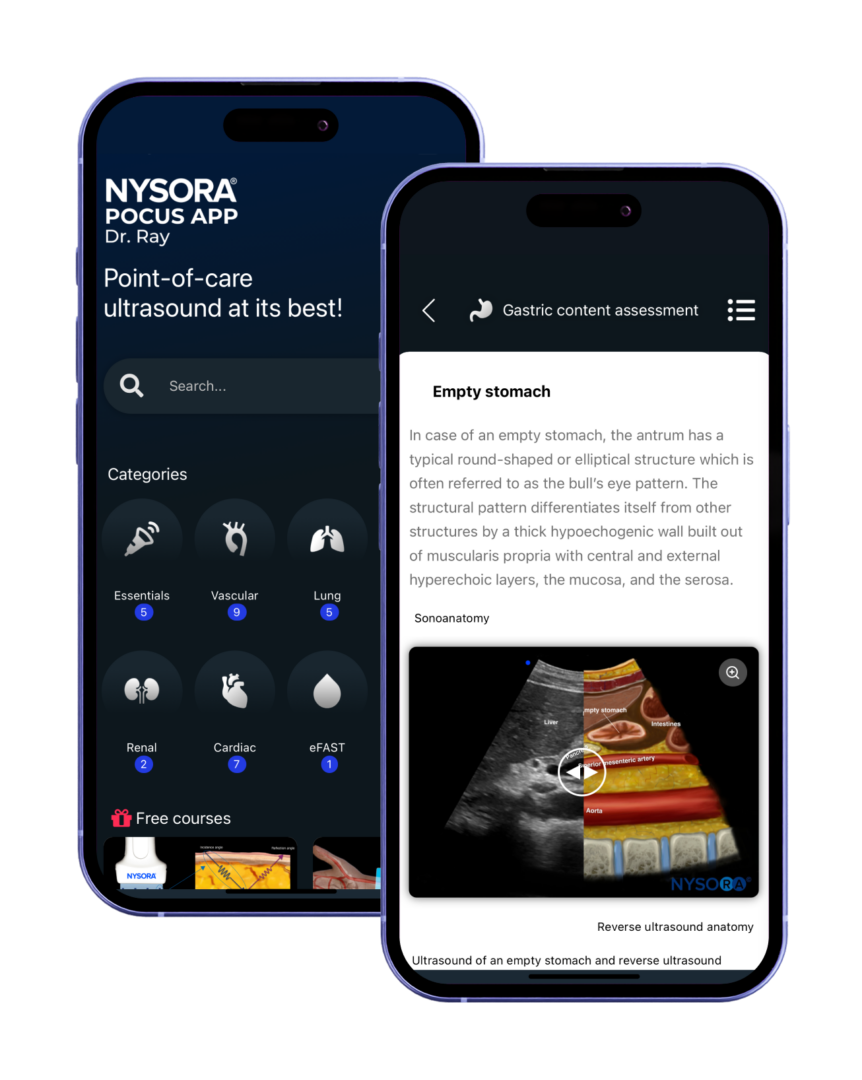
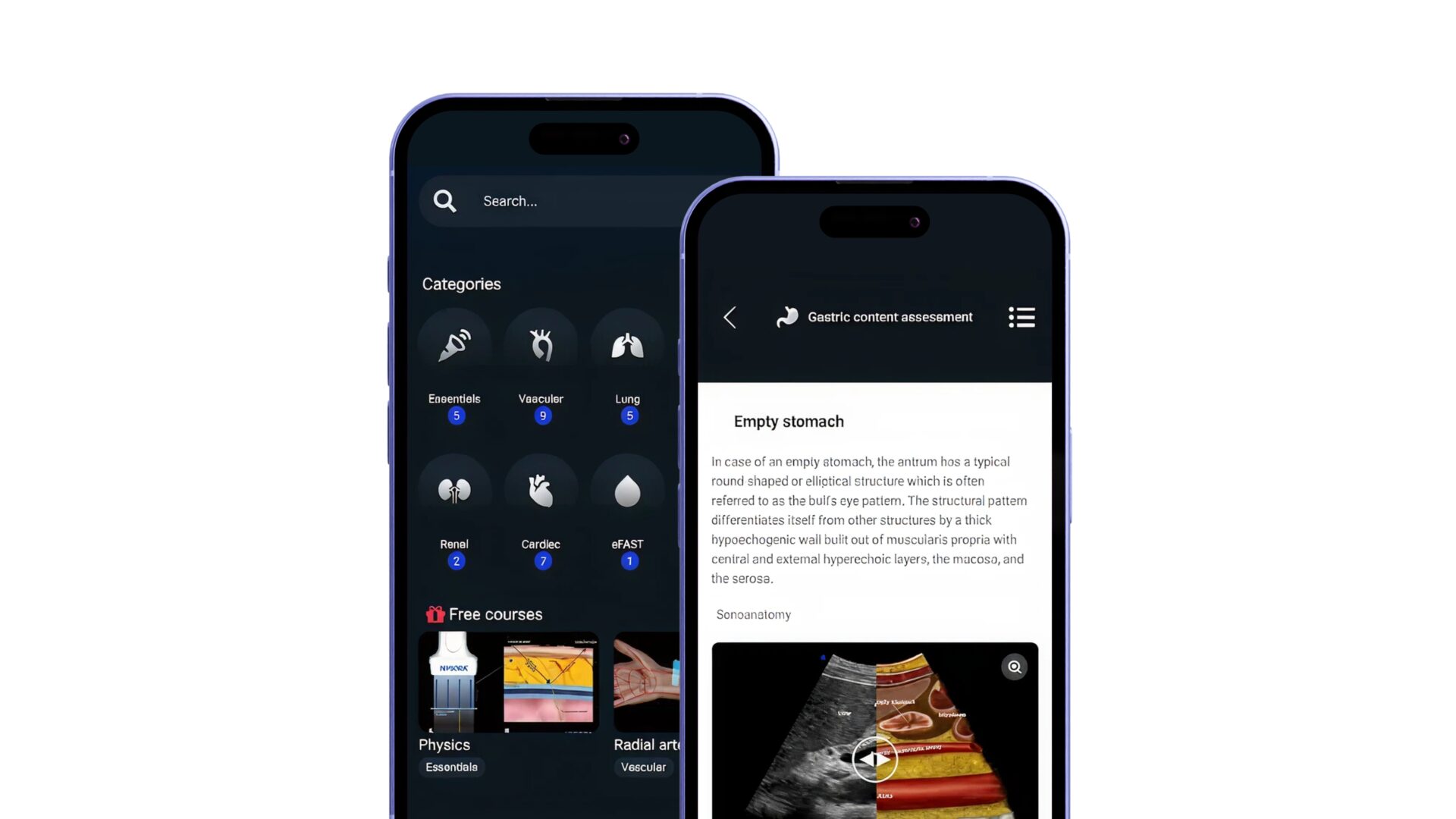
Rapid bedside diagnosis app for the heart, lungs, abdomen, vascular access, and more. Master your emergency diagnostics skills on the go!


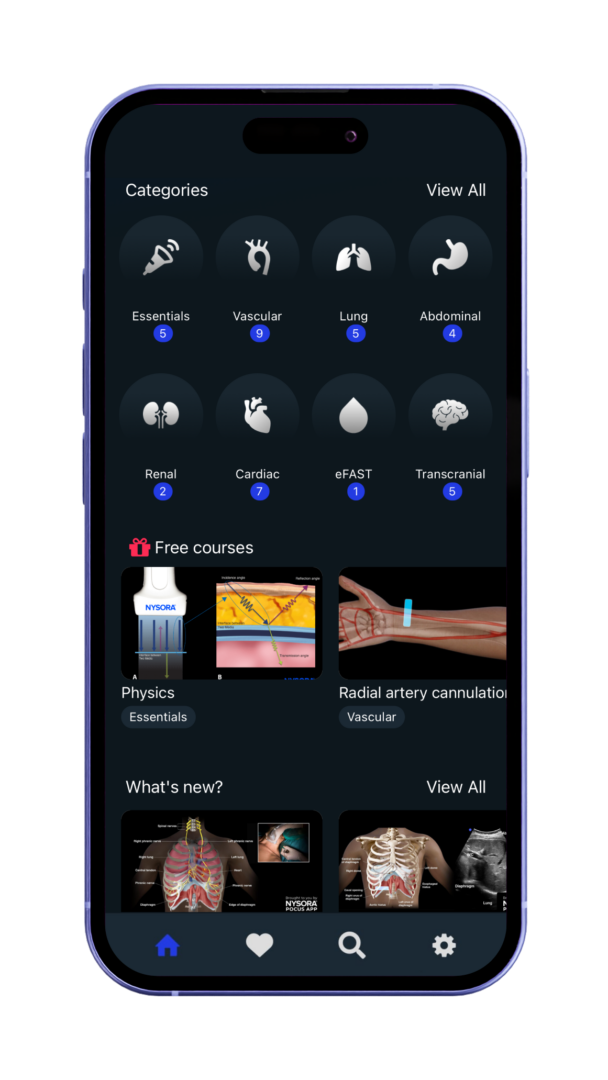
Vascular, lung, abdominal, and more.
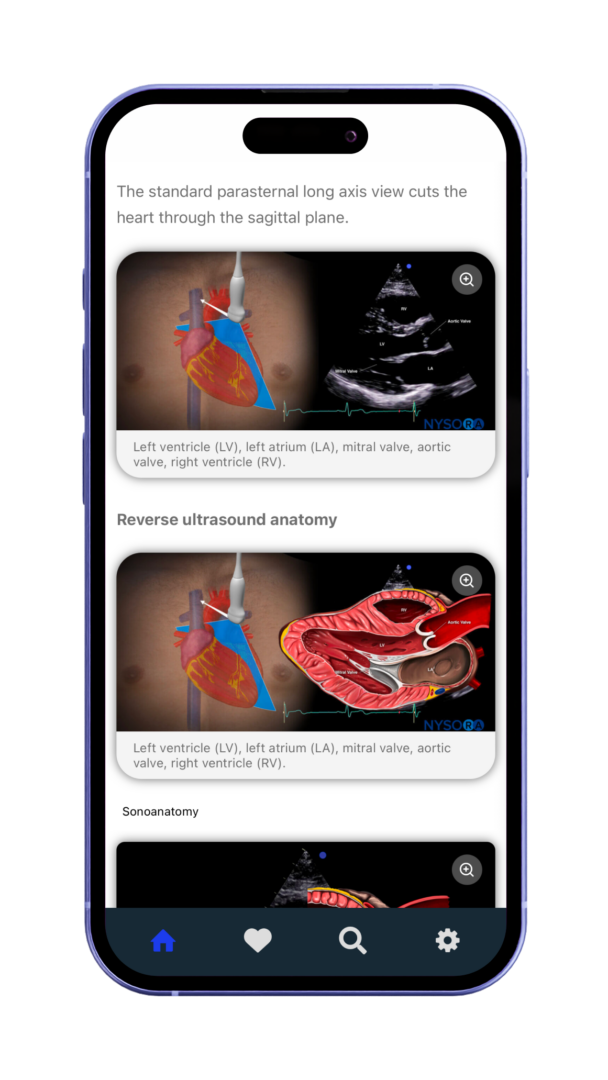
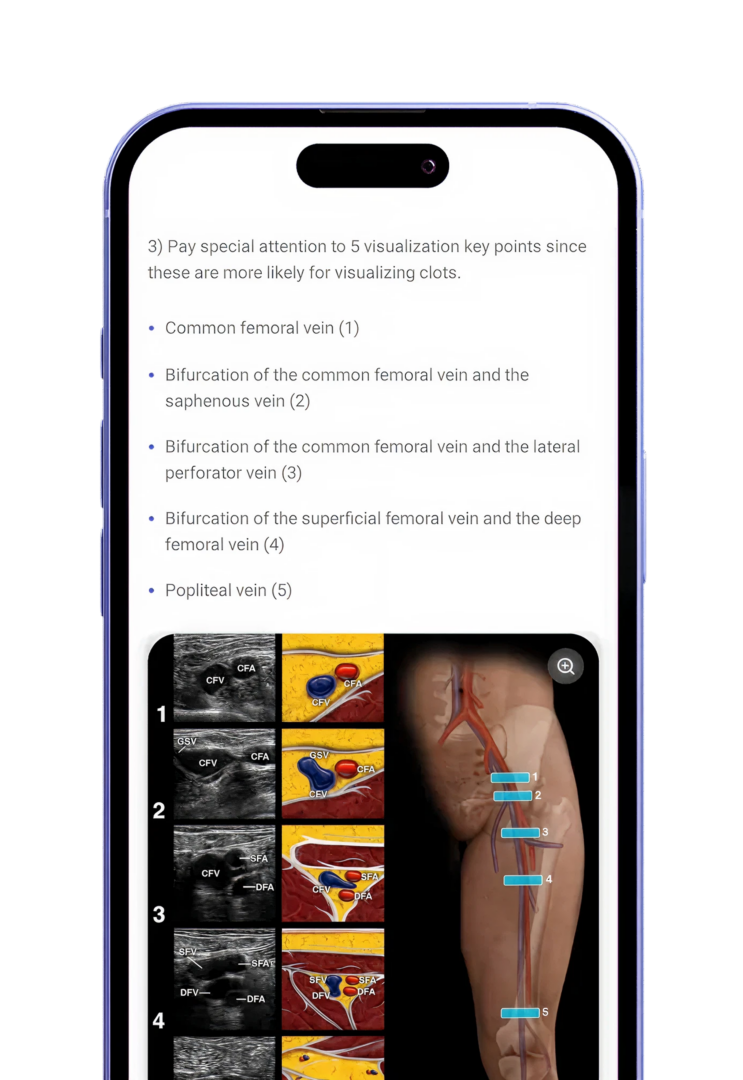
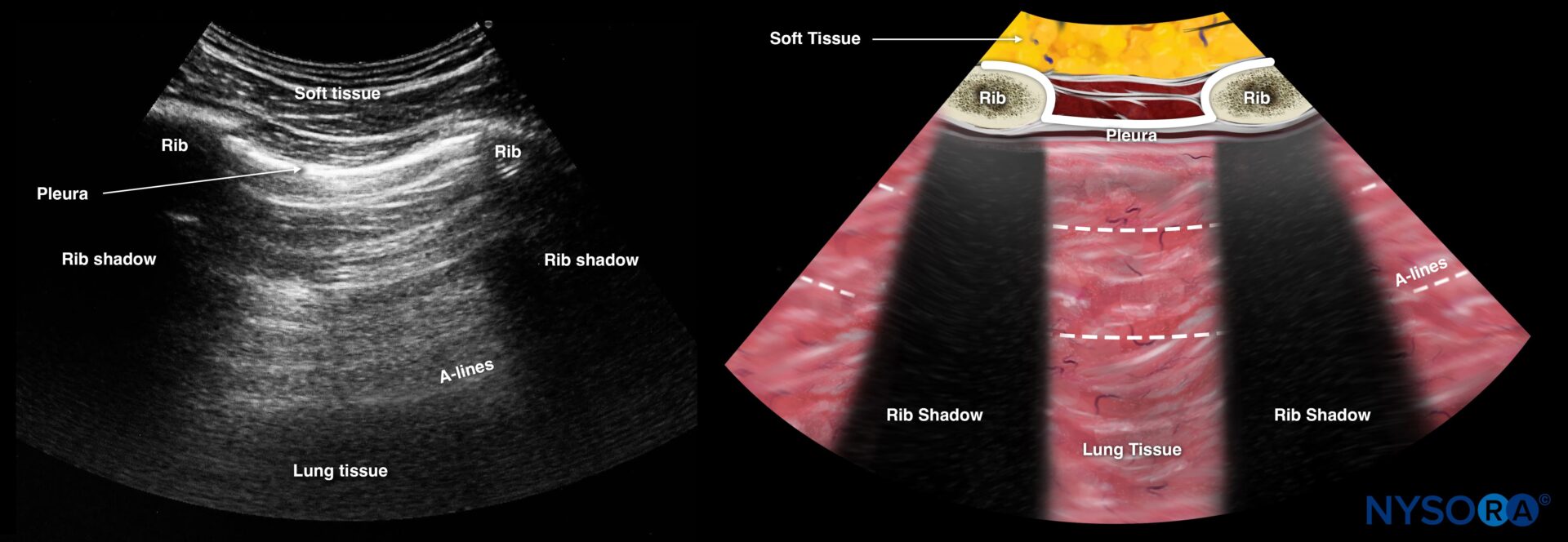
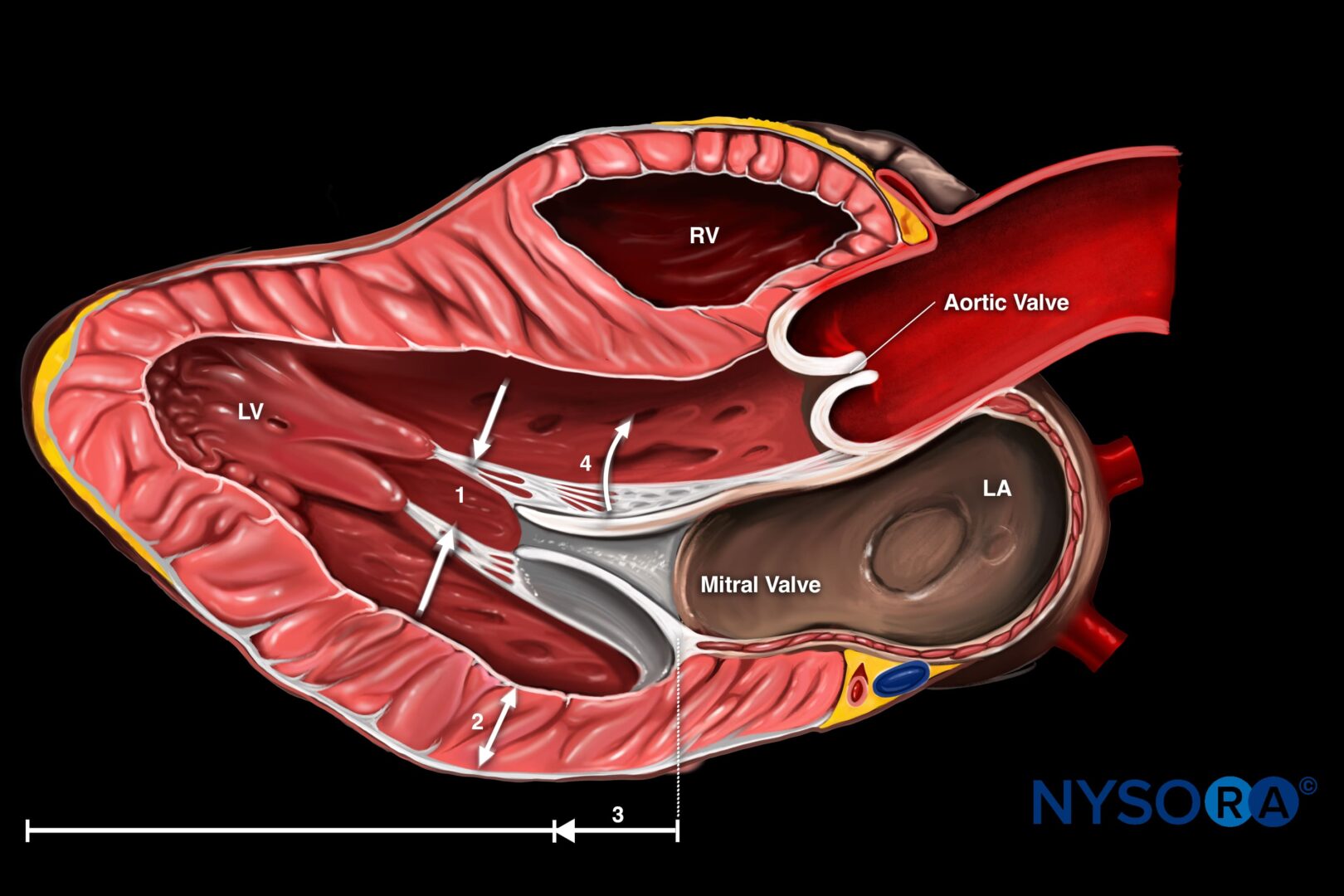
Reverse Ultrasound Anatomy illustrations make sonoanatomy easier to understand and apply.
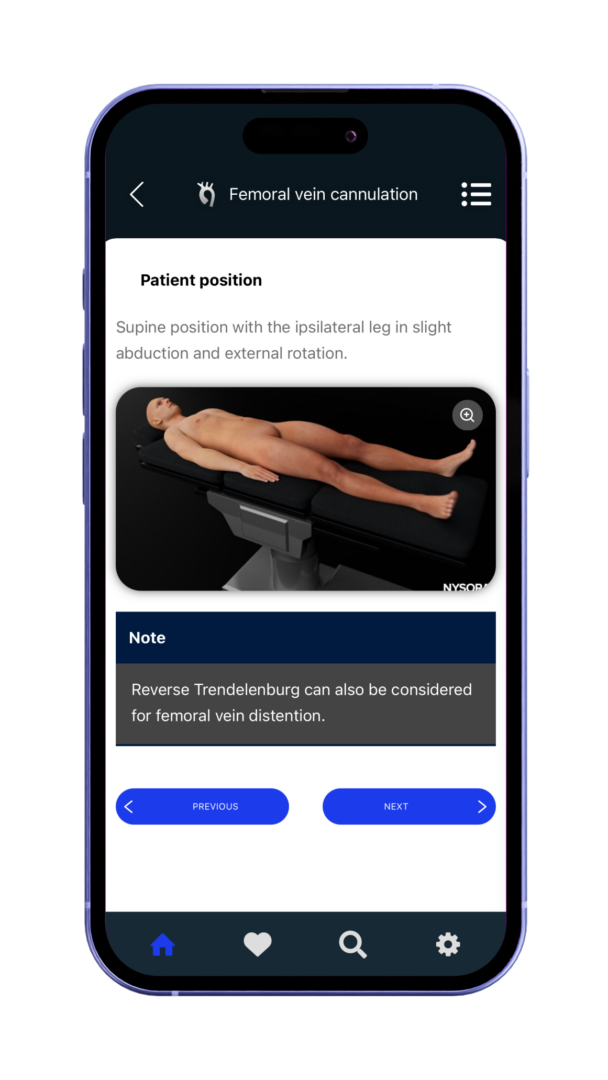
Optimized for fast, easy access on mobile and tablet devices in clinical practice.
Vascular, lung, abdominal, and more.
Reverse Ultrasound Anatomy illustrations make sonoanatomy easier to understand and apply.
Optimized for fast, easy access on mobile and tablet devices in clinical practice.
The best mobile guide for point-of-care-ultrasound. Trusted by physicians worldwide.




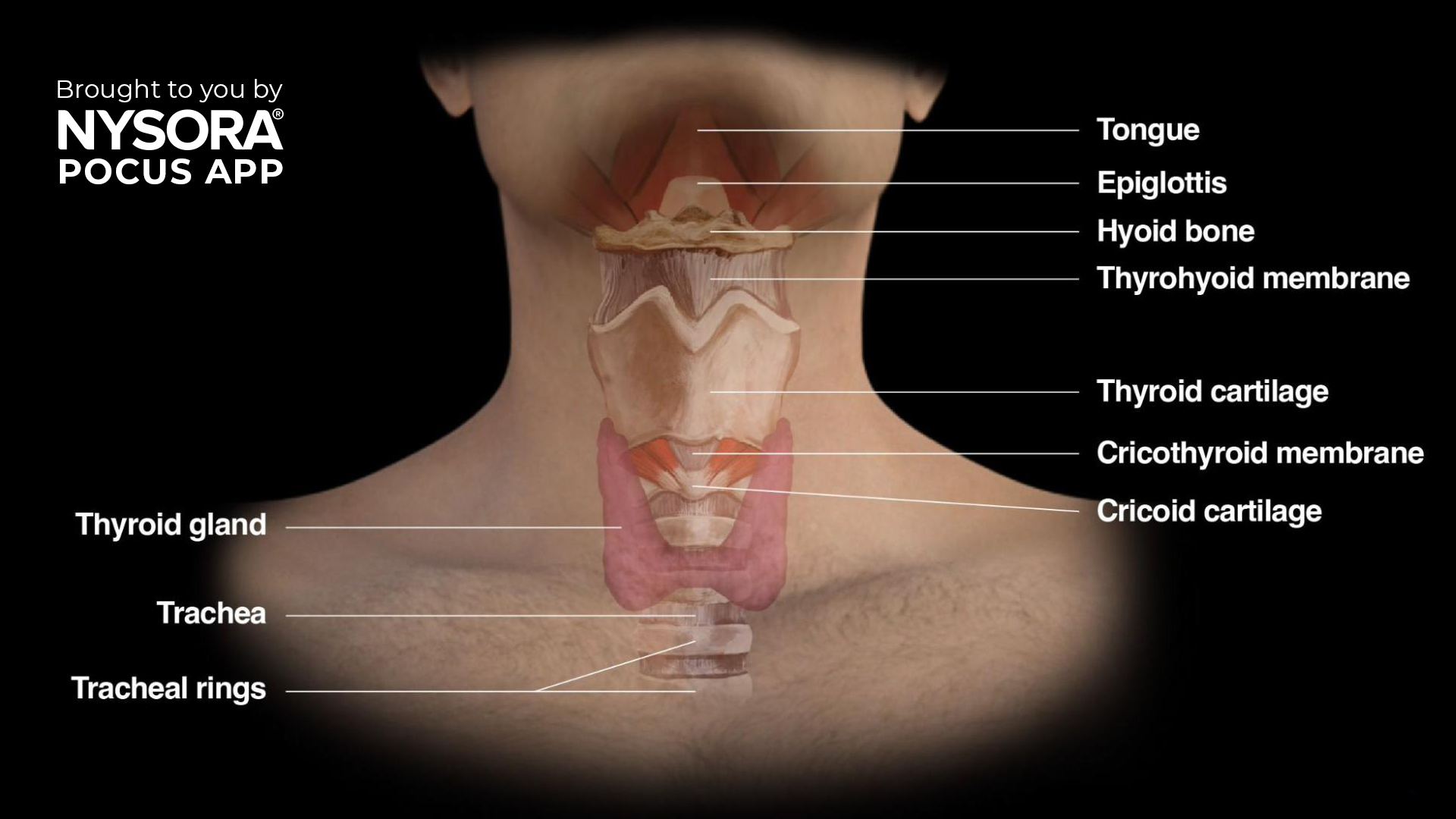
We are thrilled to announce the launch of our Airway Assessment course, now available in the POCUS App! This comprehensive course is designed to equip healthcare professionals with the knowledge and skills to perform advanced airway management using ultrasound techniques. Learning objectives You will gain expertise in: Understanding the anatomy and physiology of the upper airway. Identifying key upper airway structures. mastering the scanning techniques to assess the upper airway Why airway ultrasound? Safe and non-invasive: Quick and painless for patients. Highly accurate: Provides real-time assessment of airway structures and conditions. Improved outcomes: Reduces complications in difficult airway scenarios, a leading cause of anesthesia-related mortality. Evidence-based: Confirming ETT placement via ultrasound shows 98% sensitivity and specificity. What you’ll learn This course covers essential topics in airway ultrasound, including: Upper airway anatomy and physiology Gain a solid understanding of the functional anatomy. Identification of upper airway structures with ultrasound Detailed descriptions help you identify structures clearly, for instance: Hyoid bone – recognizable on ultrasound as a linear hyperechoic inverted U-shaped structure with two greater horns (cornua). Thyroid cartilage – ultrasound appearance as a hypoechoic inverted V-shaped or triangular structure. Cricothyroid membrane – appears as a hyperechoic horizontal line. Ultrasound imaging techniques Suprahyoid area Place the transducer longitudinally below the mandible and above the hyoid bone. Ultrasound image shows a fan-shaped tongue with a typical striated appearance. Underneath the mylohyoid and geniohyoid muscles, the tongue appears fan-shaped, with intrinsic muscles providing a striated appearance. Infrahyoid area: Sagittal ‘string of pearls’ technique Start from the trachea, sliding the probe cranially. The tracheal rings appear as dark hypoechoic structures, resembling a pearl necklace. Infrahyoid transverse approach Position the transducer transversely on the midline of the neck. Scan cranially to caudally, visualizing key landmarks: Hyoid bone Thyrohyoid membrane Thyroid cartilage Cricothyroid membrane Cricoid cartilage Trachea […]
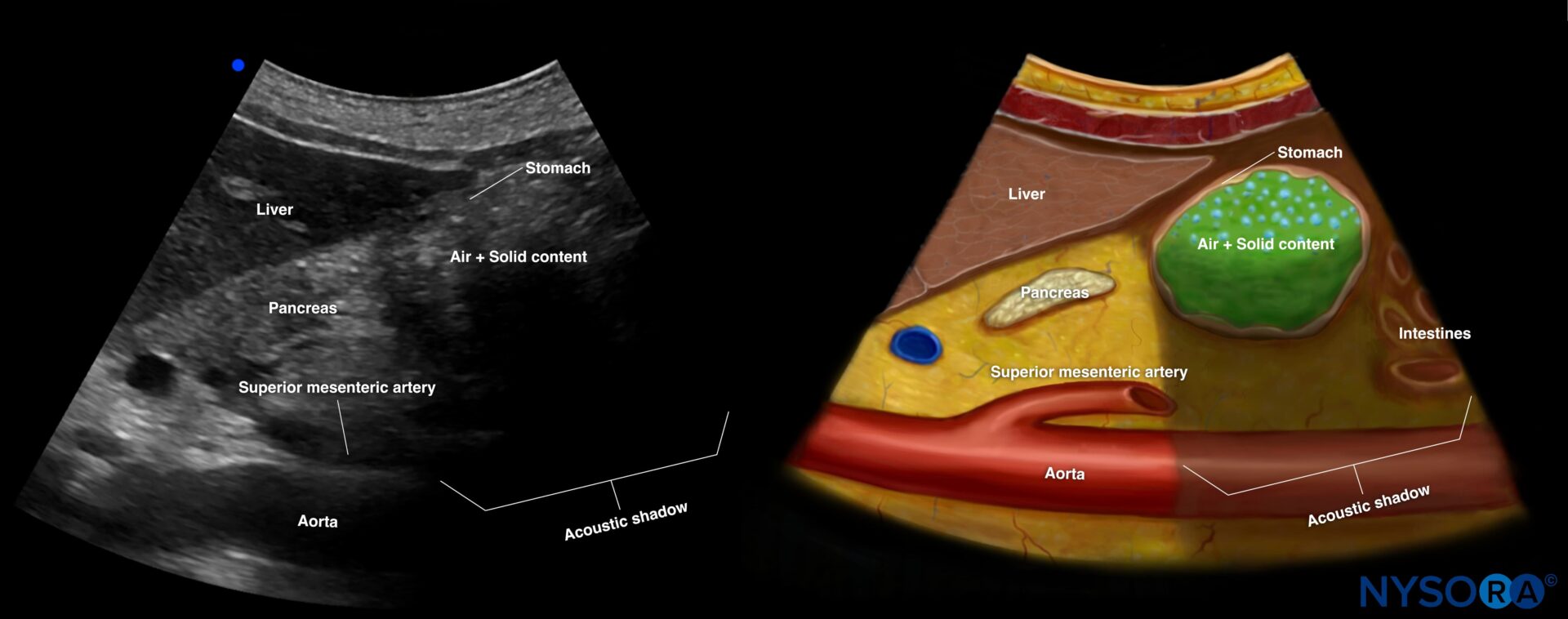
The relationship between diabetes mellitus (DM) and delayed gastric emptying has long been a concern for anesthesiologists, especially due to the associated risks of pulmonary aspiration during surgery. A recent study by Sastre et al., published in the December 2024 issue of Anesthesia & Analgesia, provides new insights into this issue by investigating the prevalence of full stomach in diabetic patients with and without dysautonomia compared to healthy controls. This landmark research highlights the importance of preoperative gastric ultrasound in risk assessment and management. Key findings Background Delayed gastric emptying is a common concern in diabetic patients due to potential autonomic dysfunction. Traditional fasting guidelines do not always account for individual variations in gastric emptying, particularly in diabetics. Study overview Participants: 289 patients undergoing elective surgery: 83 diabetics with dysautonomia. 62 diabetics without dysautonomia. 144 healthy controls. Methodology: Preoperative gastric ultrasound was performed to assess gastric volume (GV) and content. The Perlas grading scale was used to classify gastric content. Results Prevalence of full stomach: Higher in diabetic patients with dysautonomia (22.9%) compared to diabetics without dysautonomia (16.1%) and controls (13.2%). Solid gastric residue: Observed in 12% of diabetics with dysautonomia, compared to 4.8% in those without and 3.5% in controls. Gastric volume: While antral cross-sectional area (CSA) was larger in dysautonomia-positive diabetics, residual GV was not significantly different among groups. Gastroparesis symptoms: Common in diabetics with dysautonomia but not a definitive predictor of full stomach. Implications for clinical practice Role of dysautonomia: The study underscores dysautonomia as a significant factor contributing to the presence of a full stomach, rather than diabetes alone. Utility of gastric ultrasound: Ultrasound is a reliable, non-invasive tool to assess gastric contents, enabling tailored perioperative management. Guideline reevaluation: Findings suggest that current fasting guidelines may not adequately address the unique risks in diabetics with dysautonomia. […]




The best mobile guide for point-of-care-ultrasound. Trusted by physicians worldwide.
The app includes:
The NYSORA POCUS App provides quick access to expertly-curated content, helping you:
The app covers:
The app can be used in multiple ways:
It’s a mobile-friendly reference tool offering:
Join our mailing list and get weekly educational updates delivered straight to your inbox.