Explore NYSORA knowledge base for free:
Explore NYSORA knowledge base for free:
The world’s most detailed guide to ultrasound-guided regional anesthesia. Trusted by 15,000+ anesthesiologists worldwide.


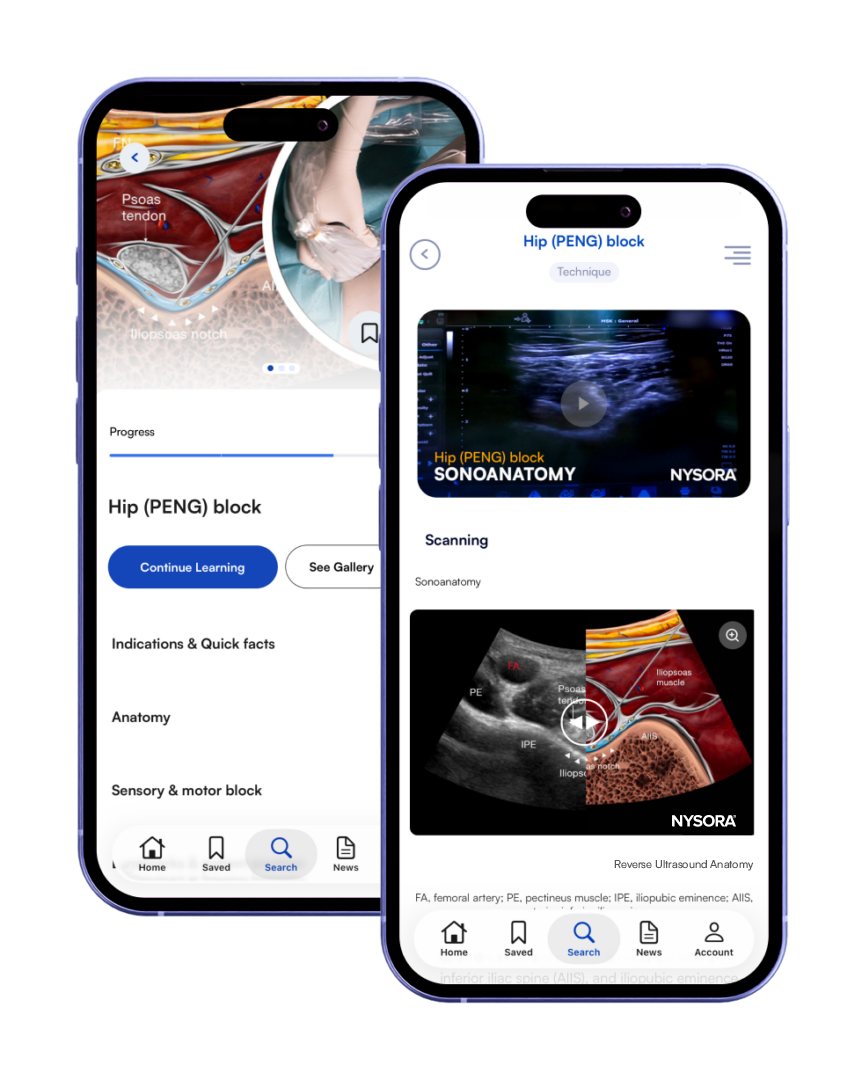
Each technique is presented in a standardized, easy-to-follow format that supports learning, teaching, and clinical performance.
Access 70+ ultrasound-guided nerve blocks and fascial plane techniques, organized by region from head to toe.

Developed by NYSORA’s clinicians and educators—combining evidence-based methodology with practical, real-world experience.
Each technique is presented in a standardized, easy-to-follow format that supports learning, teaching, and clinical performance.
Access 70+ ultrasound-guided nerve blocks and fascial plane techniques, organized by region from head to toe.
Developed by NYSORA’s clinicians and educators—combining evidence-based methodology with practical, real-world experience.
Cervical plexus block
Supraclavicular nerves selective block
Clavipectoral fascial plane block
Greater occipital nerve (GON) block
Stellate ganglion block (cervical sympathetic chain block)
Supraorbital nerve block
Infraorbital nerve block
Mental nerve block
Sub-Tenon’s (episcleral) eye block
Retrobulbar eye block
Peribulbar eye block

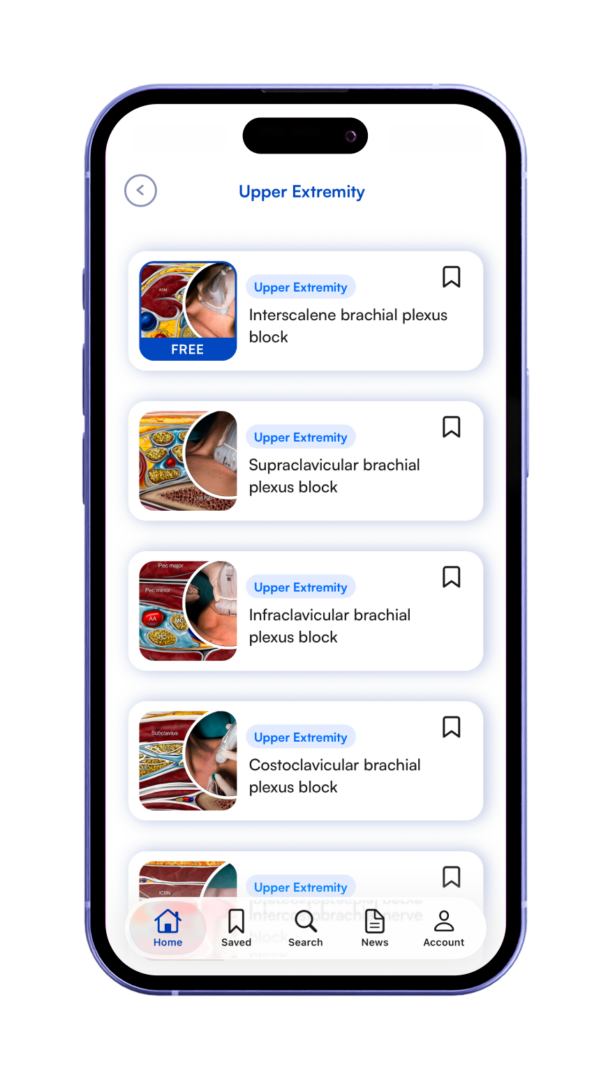
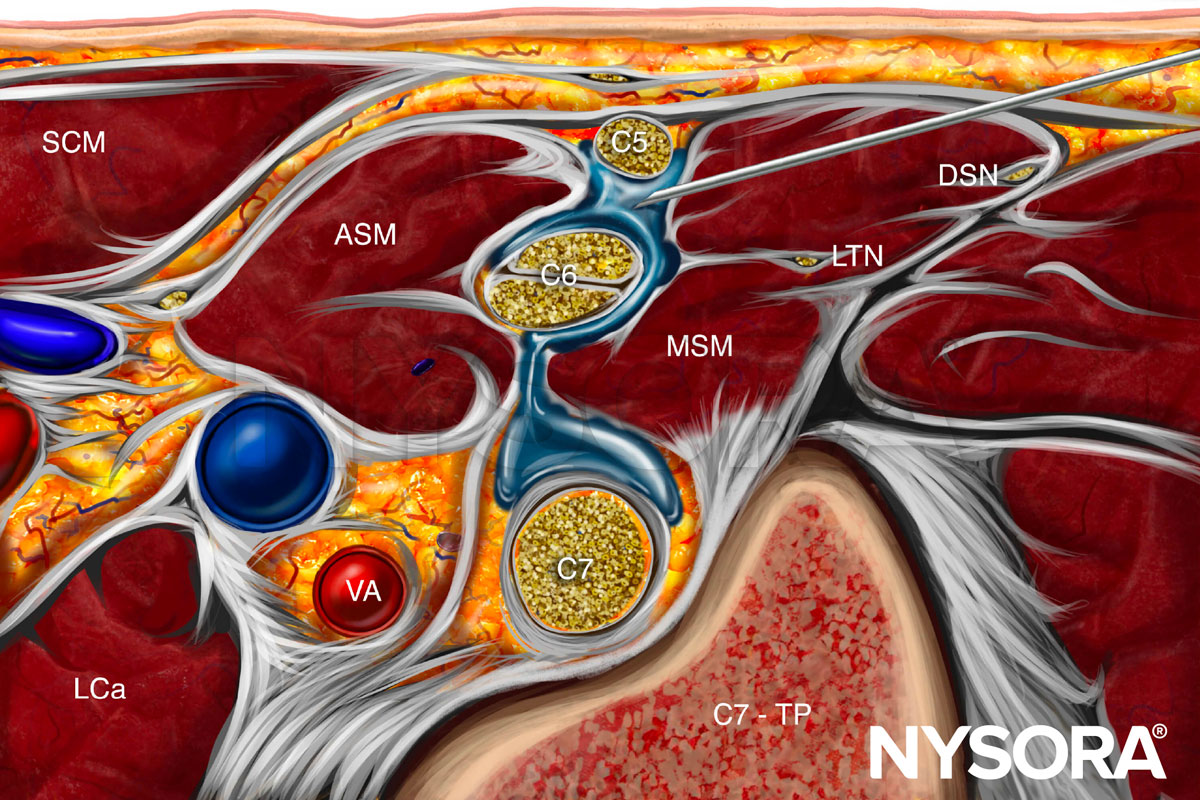
Interscalene brachial plexus block
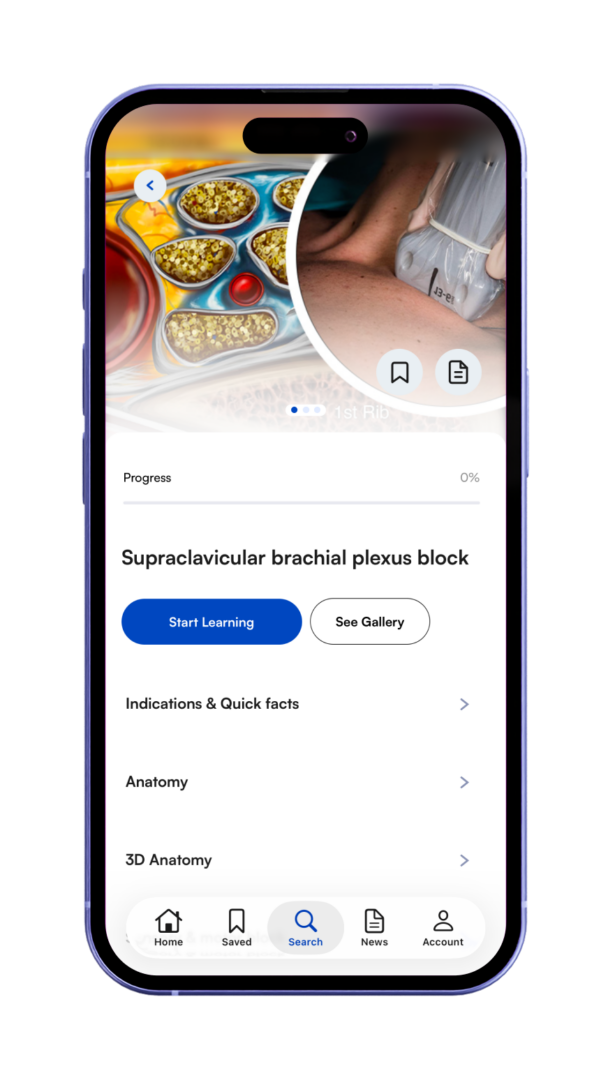
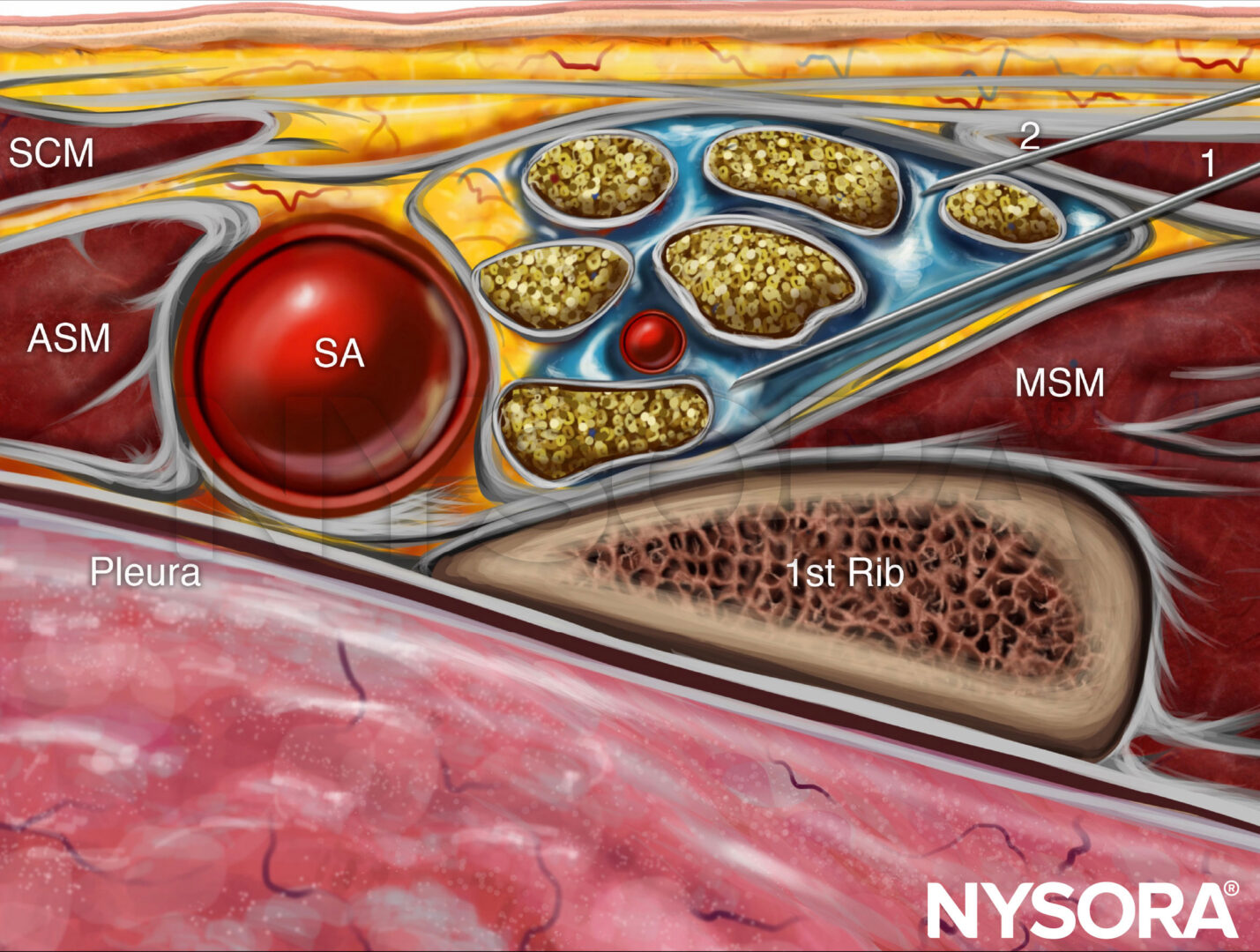
Supraclavicular brachial plexus block
Infraclavicular brachial plexus block
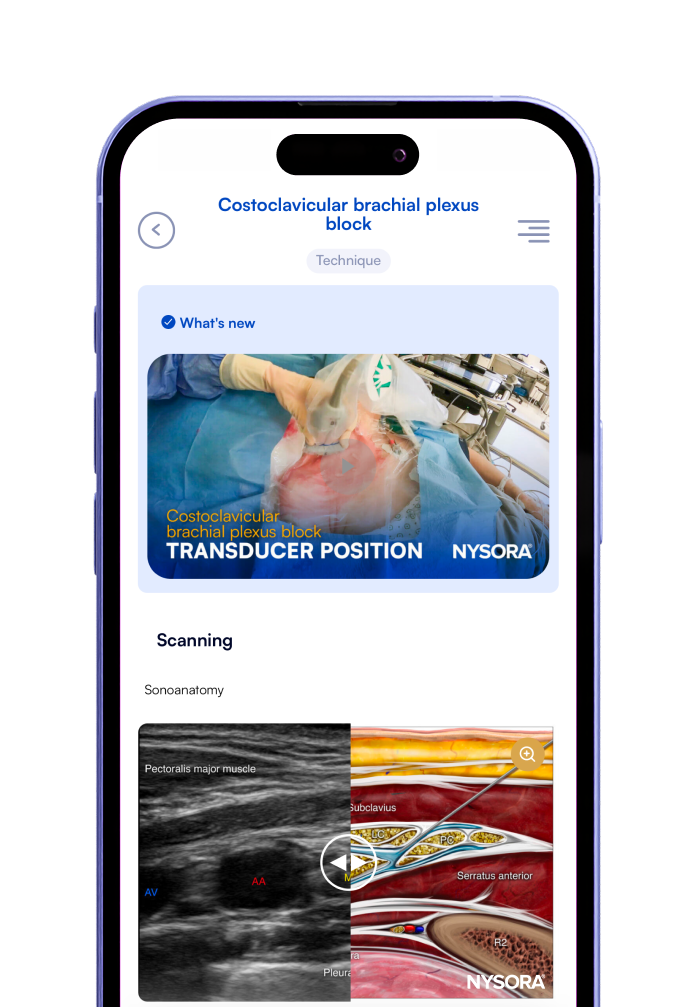
Costoclavicular brachial plexus
Intercostobrachial nerve block
Shoulder block
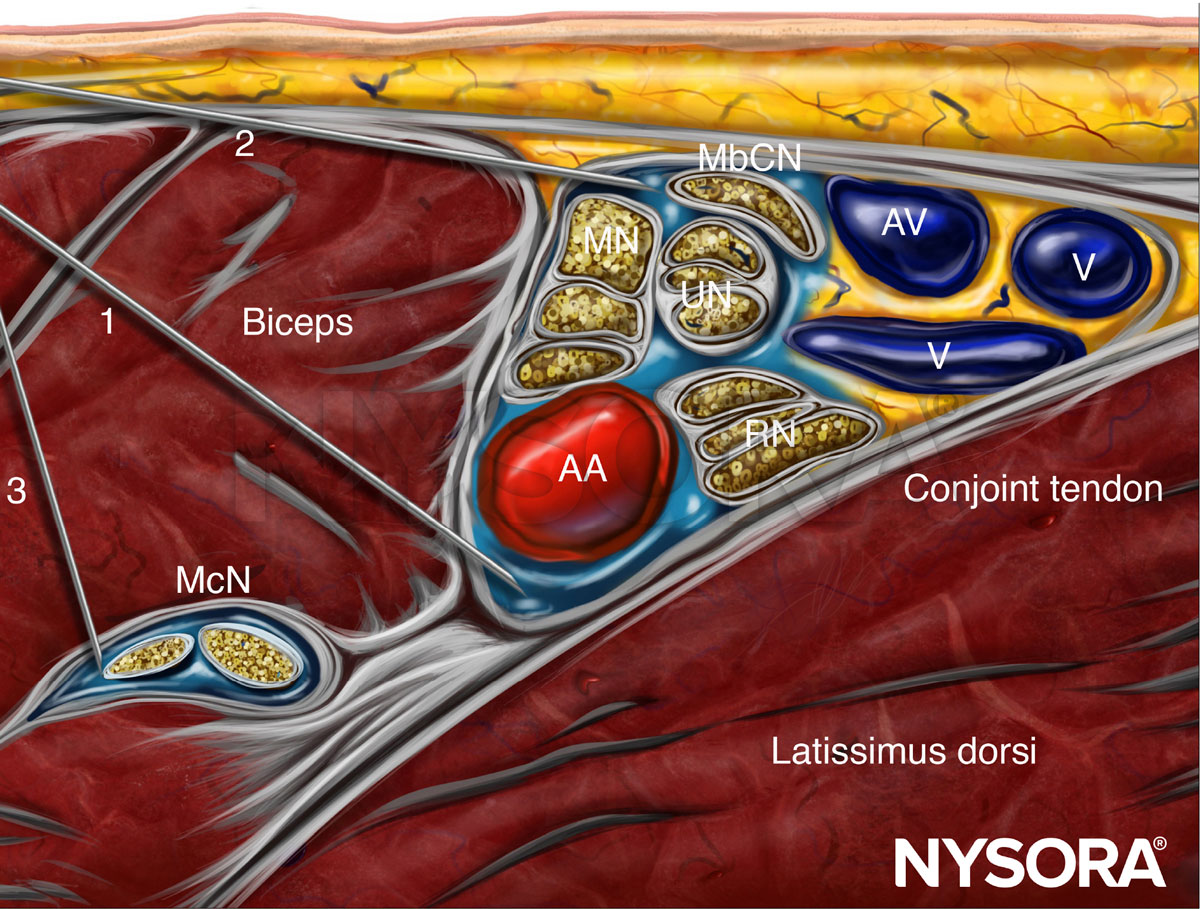
Axillary brachial plexus block
Nerve blocks above the elbow
Wrist block
Digital nerve block

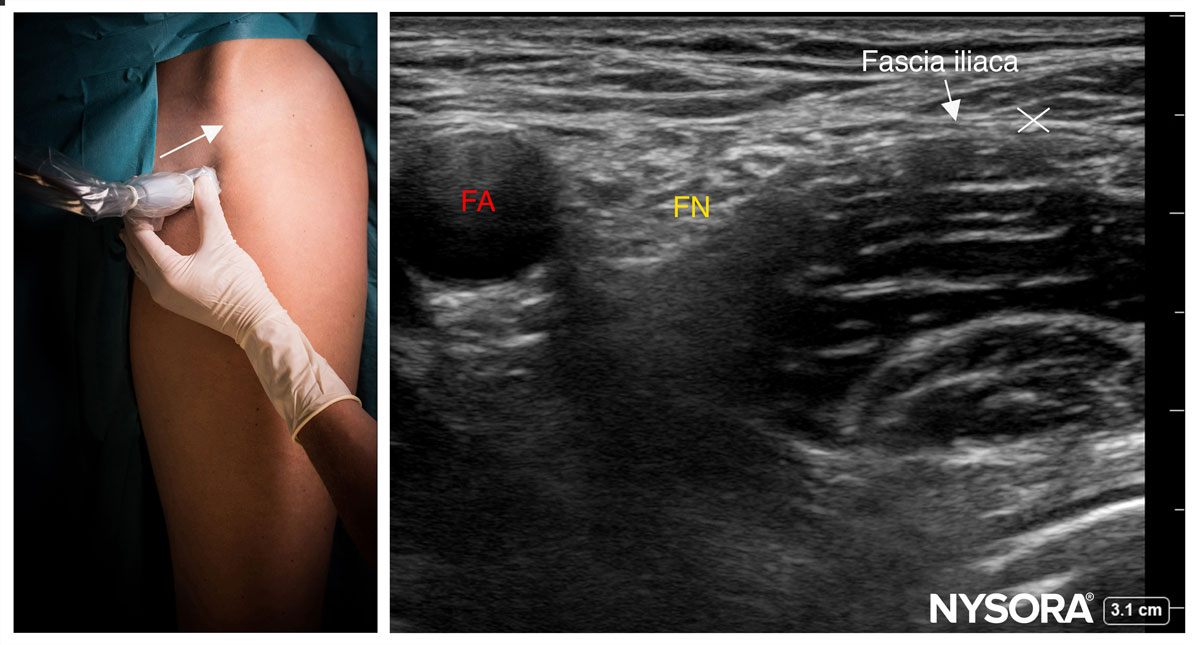
Fascia iliaca block - infrainguinal approach
Fascia iliaca block - suprainguinal approach
Hip (PENG) block
Femoral nerve block
Saphenous nerve block (adductor canal)
Femoral triangle block
Lateral femoral cutaneous nerve block
Anterior femoral cutaneous nerve block
Posterior femoral cutaneous nerve block
Obturator nerve block
Proximal sciatic nerve block
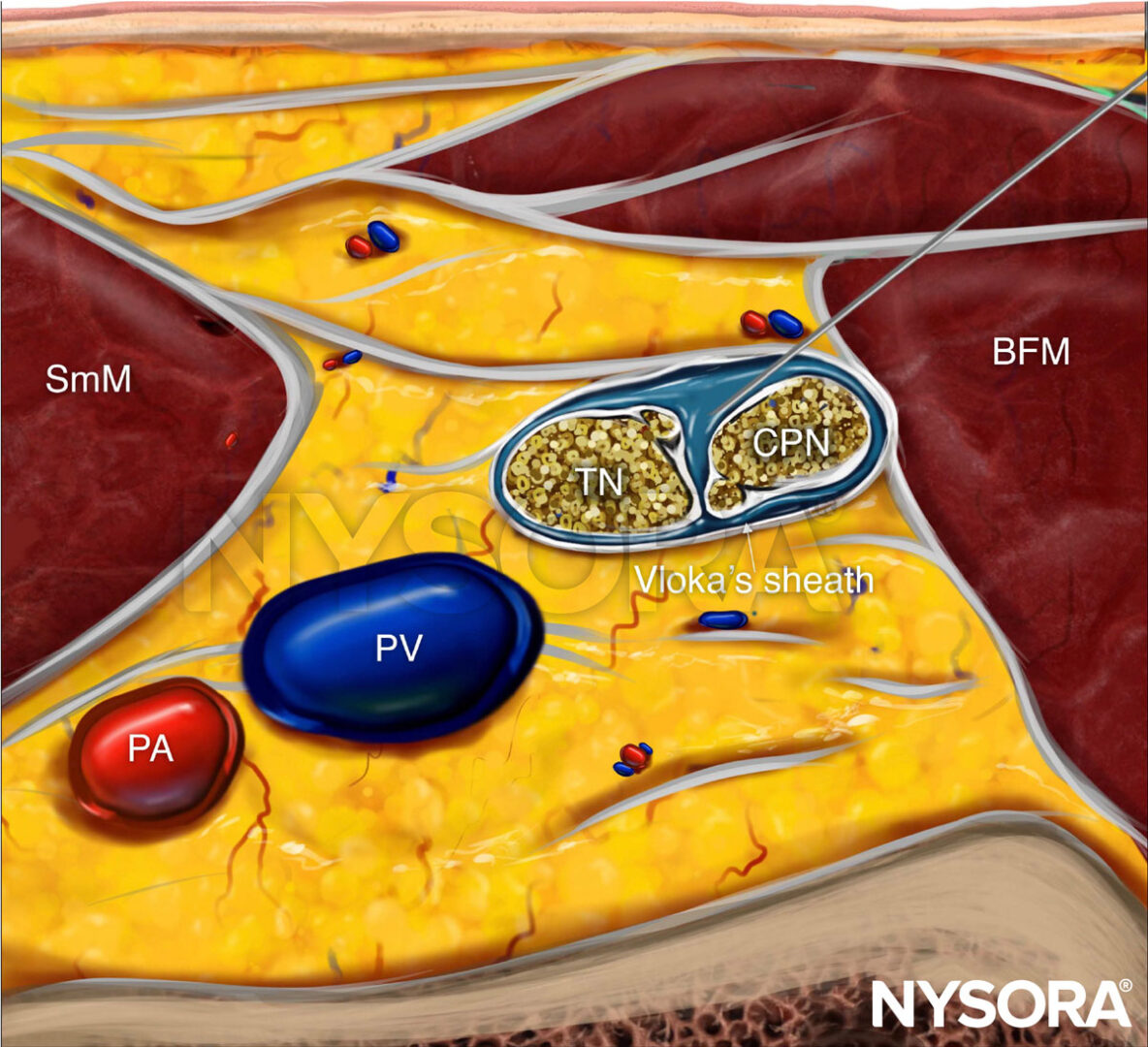
Popliteal sciatic nerve block
Genicular nerve block
IPACK block
Ankle block

Intercostal nerve block
Pectoralis and serratus plane blocks
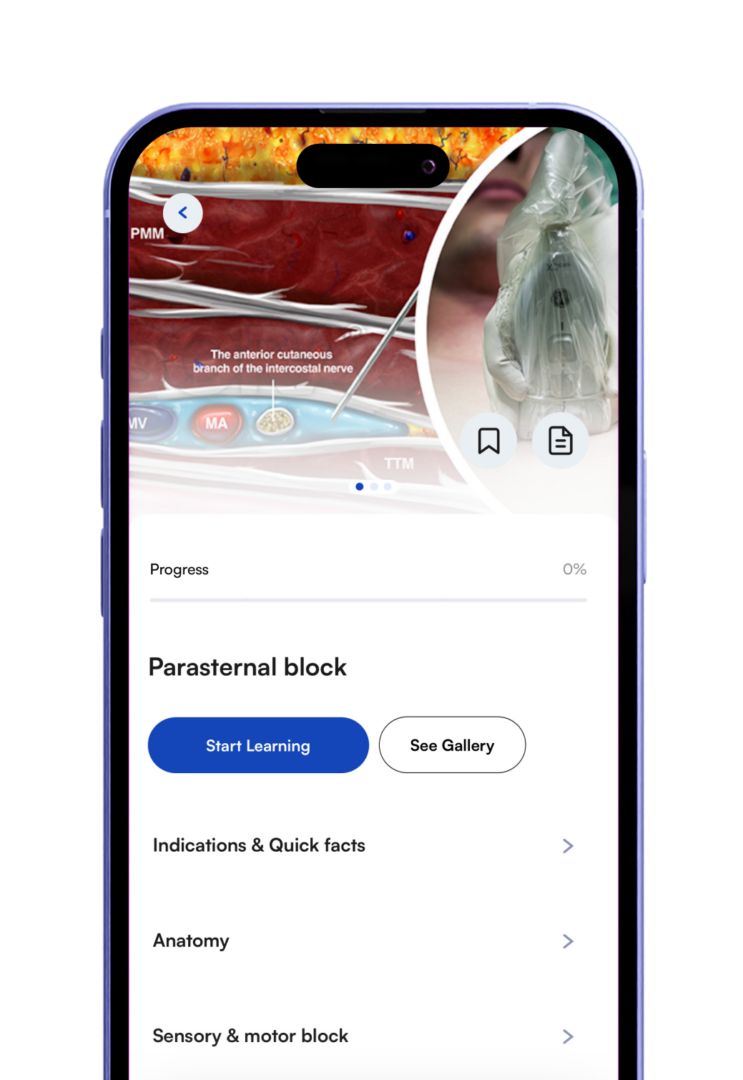
Parasternal block
Paravertebral block
Erector spinae plane (ESP) block
Transversus abdominis plane
(TAP) blocks
Ilioinguinal and iliohypogastric nerve block
Genitofemoral nerve block
Quadratus lumborum (QL) blocks
Rectus sheath block



The world's most detailed nerve blocks guide. Trusted by over 15,000 anesthesiologists worldwide.



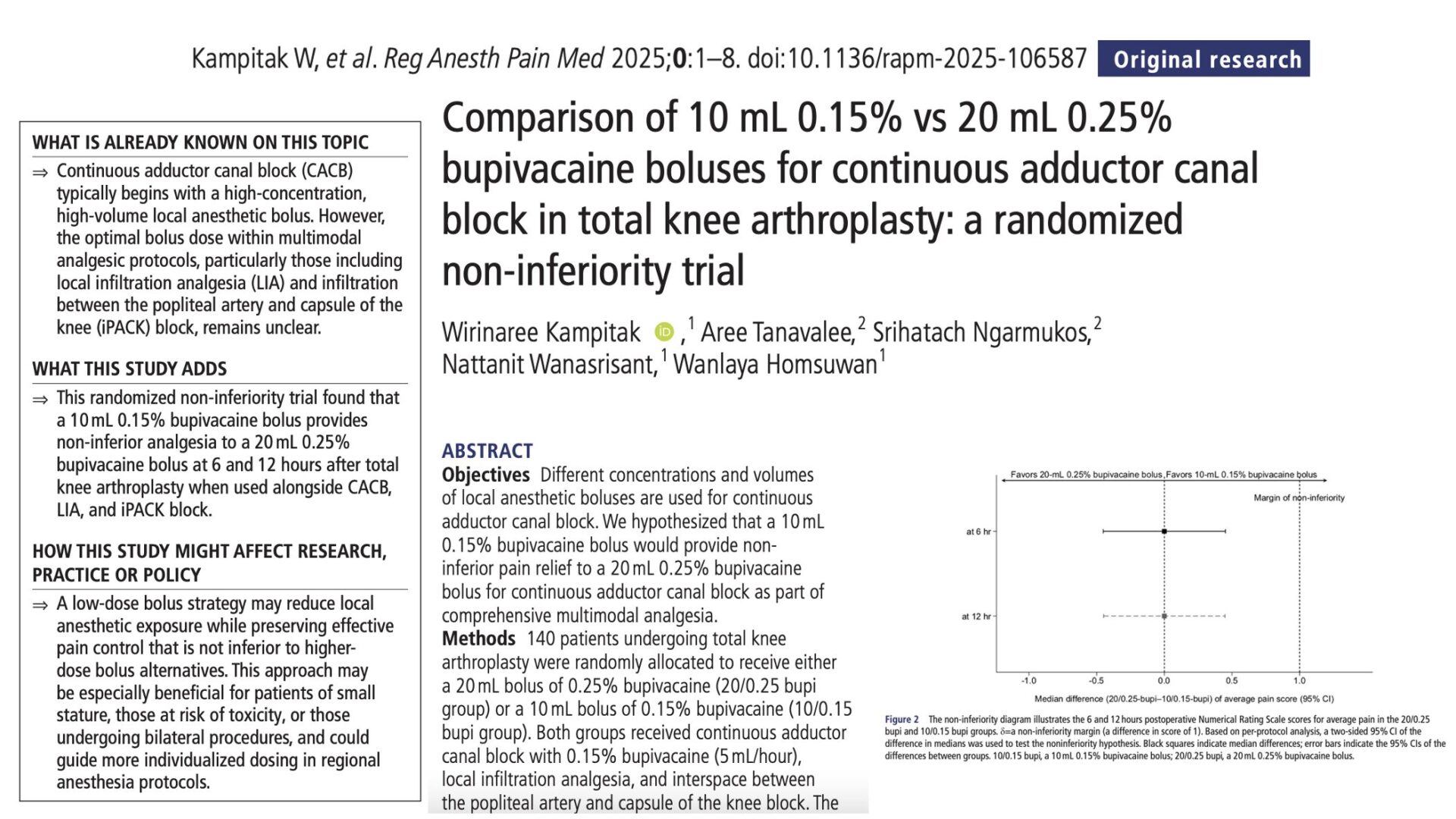
Total knee arthroplasty (TKA) is one of the most commonly performed orthopedic procedures worldwide, with increasing emphasis on enhanced recovery after surgery (ERAS) protocols. Effective postoperative analgesia is crucial to support early mobilization, reduce opioid consumption, and improve patient satisfaction. The adductor canal block (ACB) has become a cornerstone of regional anesthesia in TKA due to its motor-sparing profile and targeted analgesia of the anteromedial knee. In continuous ACB, boluses of local anesthetic are often administered via catheter to extend pain relief. However, there is little consensus on the optimal concentration and volume of local anesthetic for these boluses. This randomized non-inferiority trial, led by Kampitak et al., aimed to determine whether a low-volume, low-concentration bupivacaine bolus could provide pain relief comparable to a higher-volume, higher-concentration alternative. The results carry important implications for minimizing local anesthetic use while maintaining analgesic efficacy in TKA patients. Study objective and methods The study’s primary objective was to assess whether a 10 mL bolus of 0.15% bupivacaine is non-inferior to a 20 mL bolus of 0.25% bupivacaine in managing postoperative pain via continuous adductor canal block in patients undergoing total knee arthroplasty. This was a prospective, randomized, non-inferiority trial conducted at King Chulalongkorn Memorial Hospital in Bangkok, Thailand. The study enrolled 140 adult patients scheduled for primary unilateral TKA under spinal anesthesia, all of whom received multimodal analgesia including: Continuous adductor canal block with 0.15% bupivacaine at 5 mL/hour. Intraoperative local infiltration analgesia. A single-shot iPACK (interspace between the popliteal artery and capsule of the knee) block. Participants were randomized into two groups: 20/0.25 group: Received a 20 mL bolus of 0.25% bupivacaine. 10/0.15 group: Received a 10 mL bolus of 0.15% bupivacaine. The bolus was administered at the end of surgery through the catheter. Pain scores were assessed using an 11-point numeric rating […]
Adolescent idiopathic scoliosis (AIS) is a condition affecting 1-3% of adolescents aged 10-16, characterized by a curvature of the spine with no identifiable cause. For most patients, this condition remains mild and manageable, but in severe cases, surgical intervention through posterior spinal fusion (PSF) becomes necessary. Effective pain management following PSF is crucial to ensuring a smooth recovery and enhancing patient outcomes. Currently, multimodal analgesia, which involves combining various pain relief methods, is the standard approach. However, the role of advanced regional anesthesia techniques, such as the erector spinae plane block (ESPB), remains under-explored in pediatric populations. The ESPB is a novel regional anesthesia technique that involves injecting a local anesthetic near the spine to block pain transmission effectively. This technique has shown promising results in managing pain in adult spine surgeries and some pediatric procedures. However, its use in pediatric patients undergoing PSF for AIS has been limited. This study aimed to evaluate the practicality and effectiveness of integrating ESPB into a rapid recovery pathway for pediatric patients following PSF. Study objective and methods This prospective, randomized controlled trial enrolled 24 patients aged 10-19 years, all of whom were undergoing multilevel PSF for AIS correction. Patients were excluded if they had chronic pain conditions requiring neuromodulating medications, neuromuscular scoliosis, a history of chronic opioid therapy, or allergies/contraindications to the study medications or techniques. Participants were randomly assigned to two groups: one group of 12 patients received bilateral ESPB before the surgical incision, while the other 12 patients served as the control group and did not receive ESPB. ESPBs were administered using ultrasound guidance to inject a mixture of 0.25% bupivacaine and dexamethasone near the T7 vertebrae. Patients were evaluated at multiple time points for pain scores, satisfaction, and opioid consumption (oral morphine equivalents) during their hospital stay. The primary […]

Faster. More blocks. More videos. Continuously updated. Evidence-based. Practical.
Bring structured regional anesthesia guidance to your department.
Request Institutional AccessThe app includes:
With quick, on-the-go access to expertly-curated information, you can:
The app is designed to support you in various ways:
The app uses NYSORA’s highly standardized method. It walks you through specific, reproducible steps designed to simplify and unify your approach to nerve blocks, ensuring consistent and successful outcomes. Each technique follows the same structured format, including:
It’s a mobile-friendly reference tool offering:
Join our mailing list and get weekly educational updates delivered straight to your inbox.