Tips for a Rectus Sheath Block
The rectus sheath block provides postoperative pain relief for midline abdominal incisions. While initially used sparingly due to risks of vascular injury, the introduction of ultrasound has made the technique safer and more popular. When performed bilaterally, it effectively numbs the anteromedial abdominal wall and periumbilical area, targeting spinal dermatomes T9, T10, and T11.
For a successful rectus sheath block, adhere to the following 4 steps
- Place the transducer transversely just above the umbilicus, 1 cm lateral to the midline.
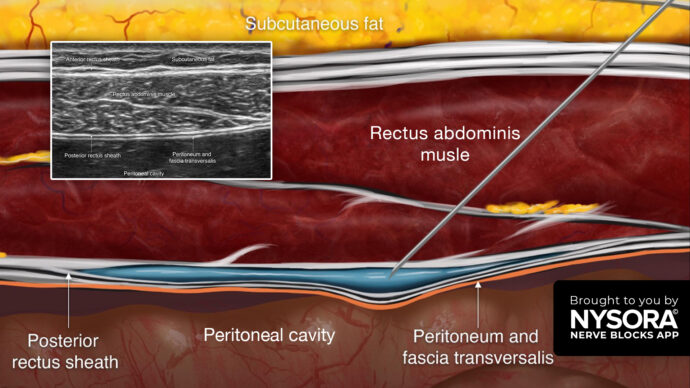
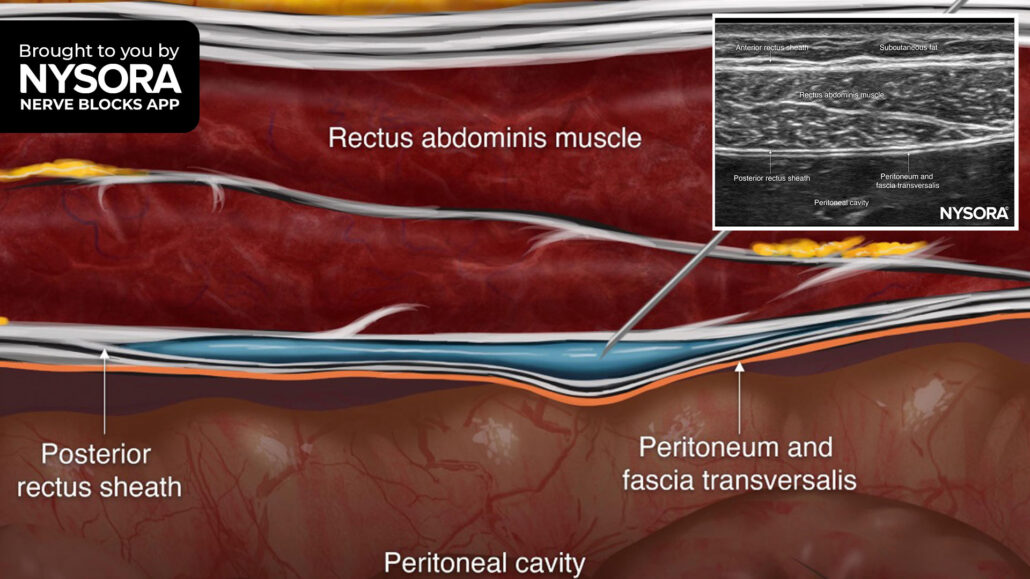
- Identify the rectus abdominis muscle and posterior rectus sheath.
- Insert the needle in-plane through the rectus abdominis muscle until the tip reaches the space between the muscle and posterior rectus sheath, and inject 10-15 mL of local anesthetic.
- Repeat on the contralateral side for a bilateral block.
Note: For optimal results, it’s important to perform the block on both sides.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!