


Learning objectives
- Recognize anesthetic complications associated with cardiac arrest
- Recognize cardiac arrest
- Treat cardiac arrest associated with anesthesia
Definition
- Advanced life support is a set of life-saving protocols and skills that extend basic life support to further support the circulation and provide an open airway and adequate ventilation (breathing)
- Is used to provide urgent treatment for cardiac emergencies such as cardiac arrest, stroke, myocardial infarction, and other conditions
- Should only be performed by paramedics and healthcare providers who have undergone more extensive training
Signs of cardiac arrest
- ECG with pulseless rhythm
- Ventricular tachycardia
- Ventricular fibrillation
- Severe bradycardia
- Asystole
- Loss of:
- Carotid pulse > 10 seconds
- End-tidal CO2 on capnograph
- Arterial line tracing
- Pulse oximeter signal
Anesthetic complications associated with perioperative cardiac arrest
- Intravenous anesthetic overdose
- Inhalation anesthetic overdose
- Neuraxial block with high-level sympathectomy
- Local anesthetic systemic toxicity
- Malignant hyperthermia
- Drug administration errors
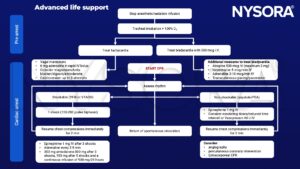
Management of cardiac arrest associated with anesthesia
Post resuscitation care
- Apply invasive monitoring
- Finalize surgical plan and transport patient to ICU
- Perform a full history and examination
- Consider therapeutic hypothermia
Keep in mind
- Defibrillation is only possible if shockable rhythm (VFIB, VTACH) occurs
- Bradycardia and hypotension under general anesthesia are relatively common
- Cardiac arrest in the peri-operative setting is relatively rare and knowing when to initiate CPR can be difficult
- CPR should be established immediately and treatment will depend on the rhythm seen by EKG monitoring
Suggested reading
- Soar J, Böttiger BW, Carli P, et al. European Resuscitation Council Guidelines 2021: Adult advanced life support [published correction appears in Resuscitation. 2021 Oct;167:105-106]. Resuscitation. 2021;161:115-151.
- Moitra VK, Einav S, Thies KC, et al. Cardiac Arrest in the Operating Room: Resuscitation and Management for the Anesthesiologist: Part 1. Anesth Analg. 2018;126(3):876-888.
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- McEvoy MD, Thies KC, Einav S, et al. Cardiac Arrest in the Operating Room: Part 2-Special Situations in the Perioperative Period [published correction appears in Anesth Analg. 2018 May;126(5):1797]. Anesth Analg. 2018;126(3):889-903.
- Moitra VK, Gabrielli A, Maccioli GA, O’Connor MF. Anesthesia advanced circulatory life support. Can J Anaesth. 2012 Jun;59(6):586-603. doi: 10.1007/s12630-012-9699-3.
We would love to hear from you. If you should detect any errors, email us at customerservice@nysora.com