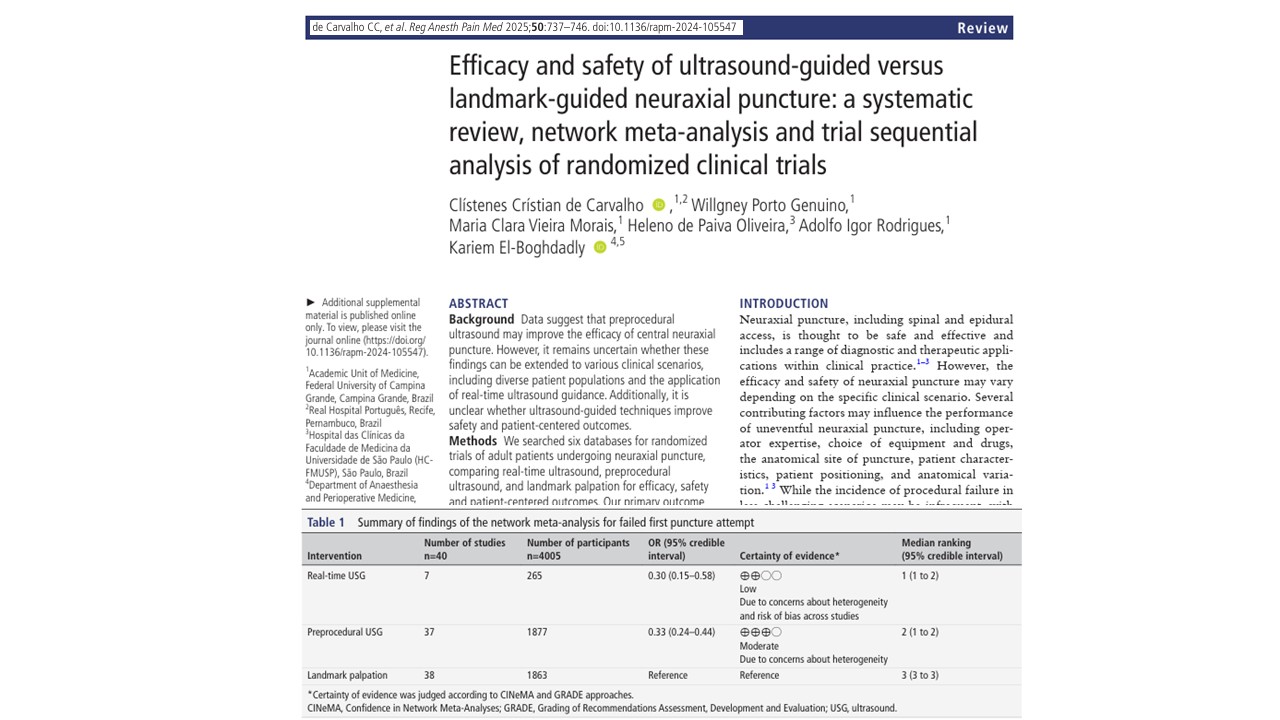

A comprehensive international systematic review and Bayesian network meta-analysis, published in Regional Anesthesia & Pain Medicine (2025), has provided definitive evidence supporting the clinical superiority of ultrasound-guided neuraxial puncture over traditional landmark-guided approaches. This large-scale analysis, encompassing 71 randomized controlled trials (RCTs) and 7,153 adult patients, found that both real-time ultrasound and preprocedural ultrasound significantly enhance the efficacy, safety, and patient-centered outcomes of neuraxial access procedures.
These findings have substantial implications for anesthetic practice, particularly for spinal and epidural anesthesia, which are foundational techniques in surgical, obstetric, and chronic pain management.
Rationale for clinical comparison
Neuraxial puncture remains a core skill in anesthesiology, employed in spinal anesthesia, epidural anesthesia, and combined spinal-epidural (CSE) procedures. While effective, these techniques can be hindered by anatomical variability, patient-specific challenges (e.g., obesity, scoliosis), and the operator’s experience.
Traditionally, practitioners rely on landmark palpation to identify intervertebral spaces. However, evidence suggests that in challenging cases, the failure rate for landmark-based puncture can reach as high as 30–40%, with increased risks of multiple attempts, needle redirections, and procedural complications.
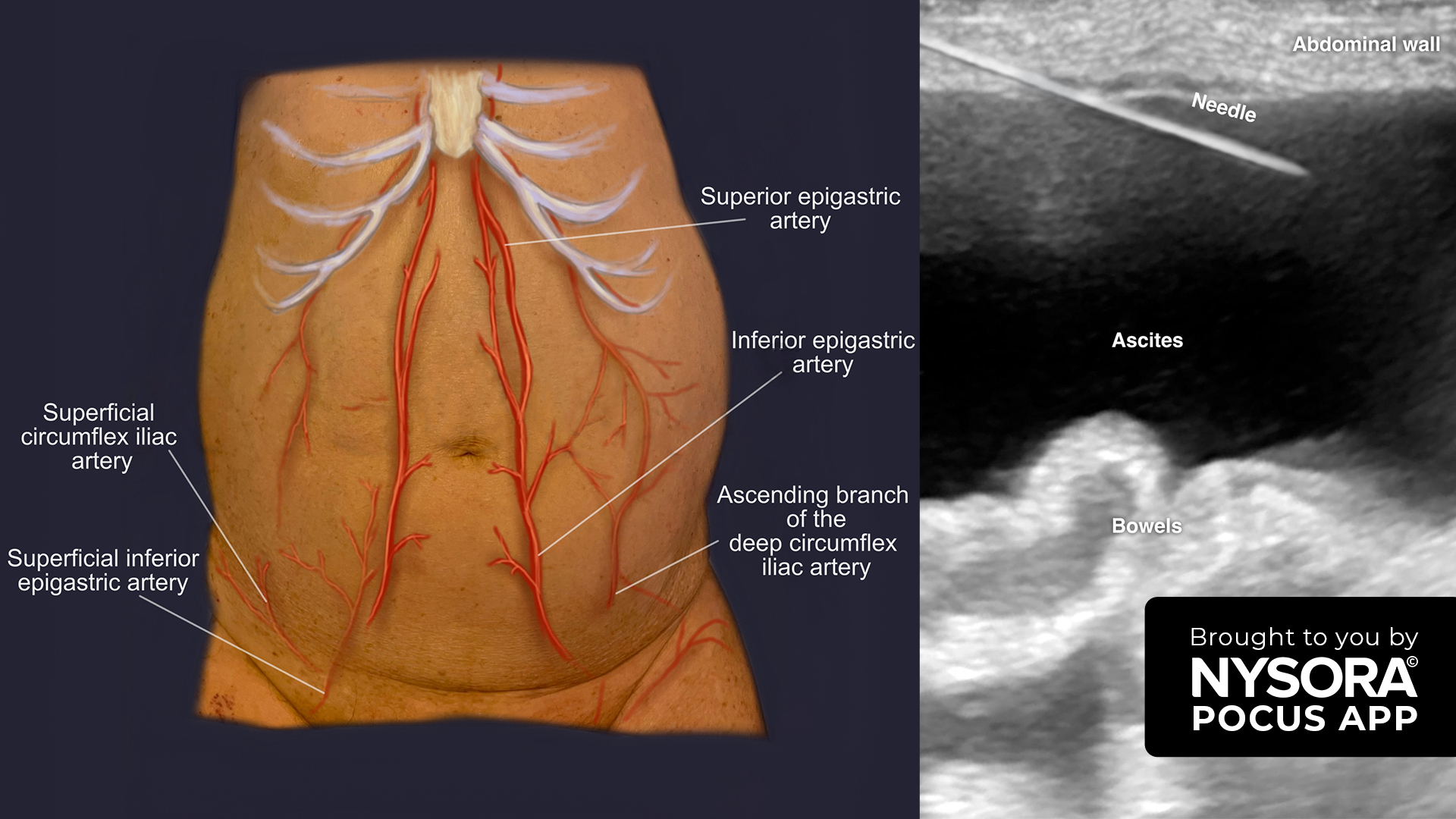
Ultrasound guidance addresses these limitations by enabling direct visualization of spinal structures, which facilitates more precise needle placement and reduces the reliance on palpation-based estimations.
Study methodology
The meta-analysis employed a Bayesian framework for network meta-analysis, supplemented by trial sequential analysis (TSA) to evaluate the cumulative evidence strength.
Key characteristics of the analysis:
- Inclusion of 71 RCTs across 21 countries (2001–2023)
- Adult patients undergoing neuraxial puncture for anesthesia, analgesia, or diagnostic interventions
- Comparison of three approaches:
- Landmark-guided palpation
- Preprocedural ultrasound
- Real-time ultrasound
Outcomes assessed:
- Primary: First-attempt failure
- Secondary: Total puncture failure, failure within two attempts, number of needle redirections, procedure time, complication rates, and patient satisfaction
The risk of bias (RoB) was assessed using the Cochrane RoB 2 tool, and the certainty of evidence was evaluated using the GRADE and CINeMA frameworks.
Key findings
Superior first-attempt success:
- Real-time ultrasound: OR 0.30 (95% CrI: 0.15–0.58); low-certainty evidence
- Preprocedural ultrasound: OR 0.33 (95% CrI: 0.24–0.44); moderate-certainty evidence
- Landmark palpation had an estimated 46.4% failure rate on the first attempt
This outcome held consistently across subgroup analyses, including:
Trial sequential analysis confirmed that the cumulative sample size achieved robust statistical power for this primary outcome.
Secondary efficacy outcomes
- Complete puncture failure: Preprocedural ultrasound reduced the risk (OR 0.29; 95% CrI: 0.11–0.61). Real-time ultrasound showed favorable trends but with broader credible intervals.
- Needle redirections:
- Real-time: −2.00 redirections (95% CrI: −3.60 to −0.35)
- Preprocedural: −1.20 (95% CrI: −1.70 to −0.72)
- Puncture time (needle-to-target): Reduced by ~30 seconds with preprocedural ultrasound
- Total procedure time: No statistically significant increase with ultrasound techniques
Patient-centered outcomes
- Satisfaction:
- Real-time ultrasound: SMD 0.74 (95% CrI: 0.20–1.20)
- Preprocedural ultrasound: SMD 0.25 (95% CrI: 0.05–0.45)
- Complications:
Accidental dural puncture: Significantly reduced with real-time ultrasound- Bloody taps: Decreased with preprocedural ultrasound (OR 0.52; 95% CrI: 0.32–0.79)
- No significant differences in postdural puncture headache, nerve irritation, or postoperative back pain
These findings align with current efforts to integrate patient-reported outcomes and safety into procedural evaluations in anesthesiology.
Broad applicability across populations
The review’s strength lies in its inclusion of diverse patient cohorts:
Even in patients considered low-risk for puncture failure, ultrasound provided statistically and clinically significant benefits, undermining the perception that it is only necessary in “difficult” cases.
Procedural implications and clinical recommendations
The cumulative evidence advocates for the integration of ultrasound as a standard adjunct to neuraxial anesthesia. Notably:
- Real-time ultrasound yielded the highest rankings for reducing puncture attempts, needle redirections, and complications.
- Preprocedural ultrasound offered similar advantages, particularly in resource-constrained settings or where real-time imaging is impractical.
Both modalities improve clinical outcomes with no significant increase in procedure duration, reinforcing their utility in both elective and urgent cases.
Limitations and future directions
While the evidence is strong, the authors acknowledge several limitations:
- Fewer studies on thoracic epidurals limit generalizability in this region
- Operator experience was variably reported and may influence outcomes
- Economic evaluations were not included, and real-world implementation data are lacking
- The results primarily reflect technical performance, not full anesthesia success
Future research should:
- Compare real-time vs. preprocedural ultrasound in head-to-head trials
- Investigate cost-effectiveness and implementation strategies
- Assess ultrasound’s role in thoracic and emergency neuraxial access
Conclusion
This systematic review and meta-analysis provide moderate to high-quality evidence that ultrasound-guided neuraxial puncture enhances clinical efficacy, reduces procedure-related complications, and improves patient satisfaction. While the relative superiority of real-time versus preprocedural ultrasound remains to be conclusively determined, the evidence robustly supports routine integration of ultrasound guidance in clinical practice for spinal and epidural procedures. This evidence-based shift challenges the continued reliance on landmark palpation, particularly in high-risk populations, and positions ultrasound as the new standard for safe, effective, and patient-centered neuraxial anesthesia.
For more information, refer to the full article in RAPM.
de Carvalho CC, Porto Genuino W, Vieira Morais MC, de Paiva Oliveira H, Rodrigues AI, El-Boghdadly K. Efficacy and safety of ultrasound-guided versus landmark-guided neuraxial puncture: a systematic review, network meta-analysis and trial sequential analysis of randomized clinical trials. Reg Anesth Pain Med. 2025 Sep 4;50(9):737-746.
Read more about neuraxial anesthesia in our Regional Anesthesiology Module on NYSORA 360—a complete training resource designed for residents, with practical, up-to-date guidance on perioperative and critical care management.