An interscalene brachial plexus block anesthetizes the brachial plexus at the level of the roots and results in anesthesia of the shoulder, upper arm, and lateral two-thirds of the clavicle.
We wanted to share these 4 tips to perform an interscalene brachial plexus block successfully
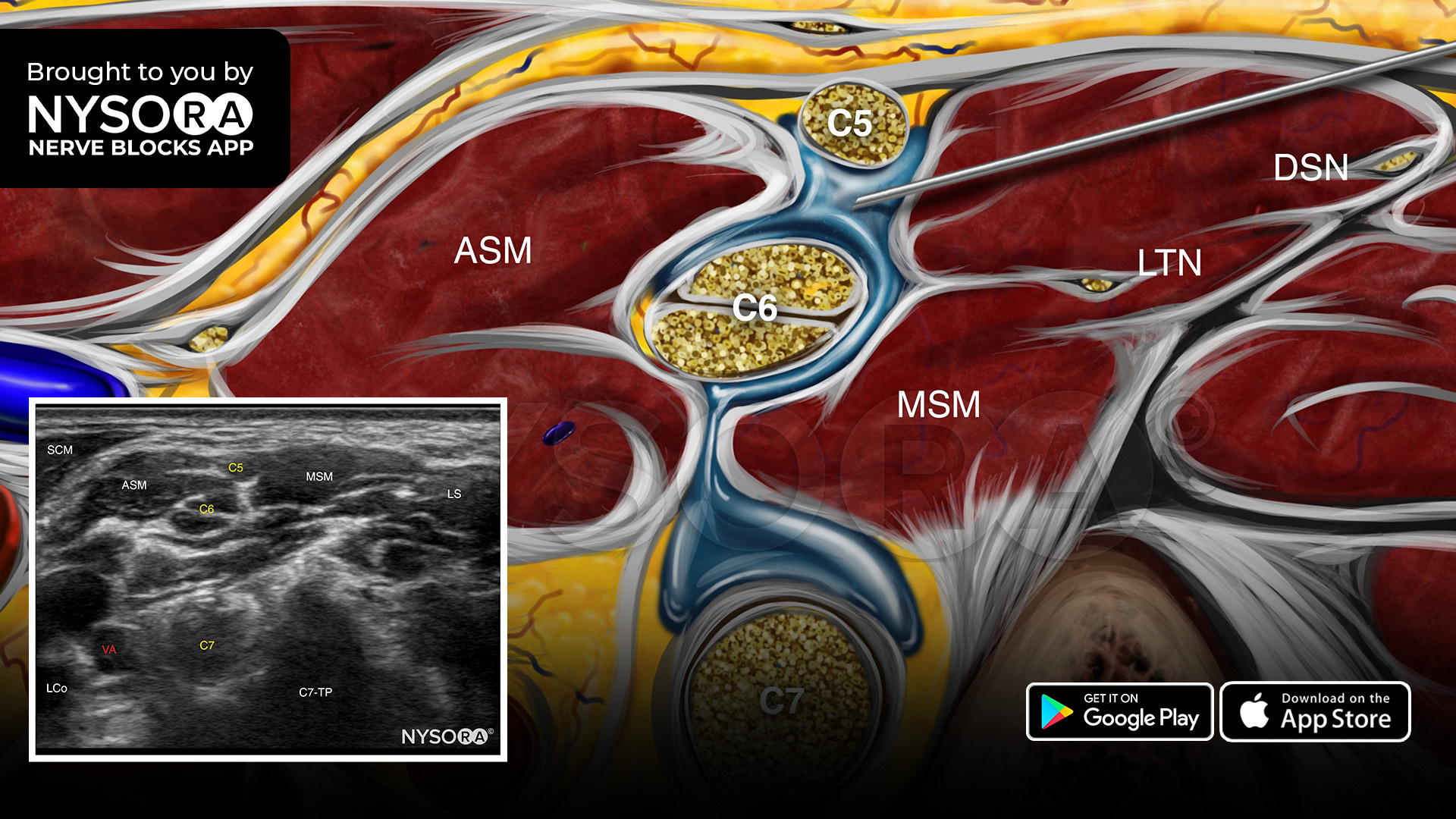
- Place the transducer at the supraclavicular fossa to identify the brachial plexus. Trace the supraclavicular brachial plexus to the level of the interscalene space.
- Insert the needle in-plane, from lateral to medial, to inject 7-15 mL of local anesthetic around the superior trunk (i.e., C5 and C6 rami) and middle trunk (i.e., C7 ramus) of the brachial plexus in the interscalene space between the anterior and middle scalene muscles.
- Aim the needle between the roots to decrease the risk of accidental nerve injury.
- A proper spread, inside the sheath, will result in displacement of the brachial plexus by the local anesthetic.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE.