Nerve Block Tip of the Week: Posterior TAP block
A posterior transversus abdominis plane (TAP) block is a common and relatively simple regional anesthetic procedure, but there are a few things that you can do to ensure its success. As part of our “Nerve Blocks from the App” series, we’re sharing everything you need to know about it to get started.
A posterior TAP block anesthetizes the anterior and sometimes lateral abdominal wall between the costal margin and iliac crest (T9-T12).
Here are 3 tips that will help you to successfully perform a posterior TAP block:
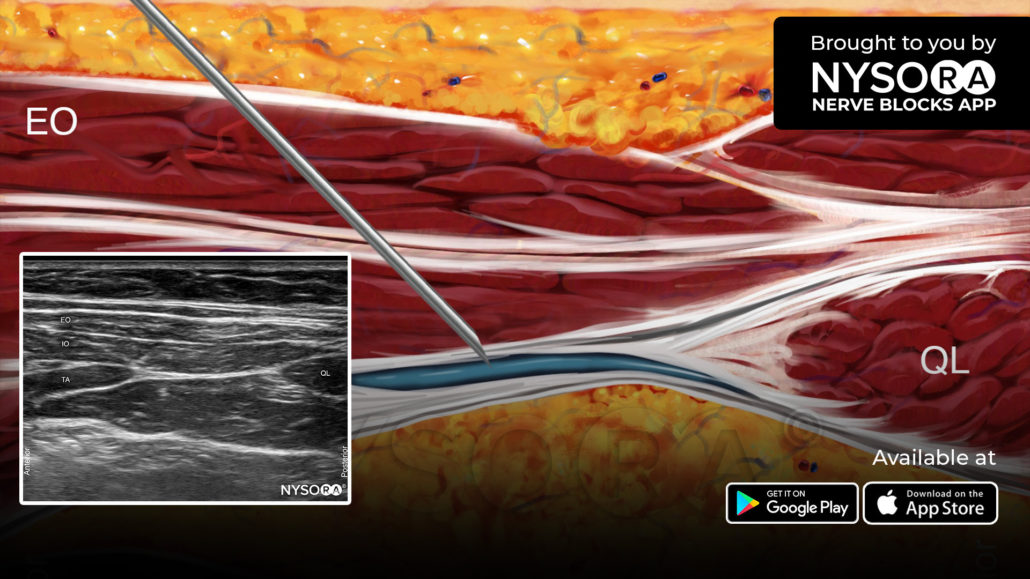
- Place the transducer in an axial orientation over the midaxillary line and scan posteriorly following the fascial plane between the internal oblique and transversus abdominis muscles.
- Identify the posterior border of the transversus abdominis plane.
- Insert the needle in the midaxillary line and continue in the posterior direction until it reaches the end of the transversus abdominis plane, and then inject 15-20 mL of local anesthetic.
Watch the video below to better understand the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, learn more about the Nerve Blocks App HERE.