Tips for the Popliteal Sciatic Nerve Block
The popliteal sciatic nerve block is indicated for foot and ankle surgery, foot and toe amputation, and Achilles tendon surgery. It targets the sciatic nerve at or slightly above its division into the tibial and common peroneal nerves. The block can be used alone or combined with femoral or saphenous nerve blocks. Unlike more proximal approaches to the sciatic nerve, this technique preserves hamstring motor function, but foot drop remains a potential issue.
Achieving a successful popliteal sciatic nerve block involves these 3 essential steps
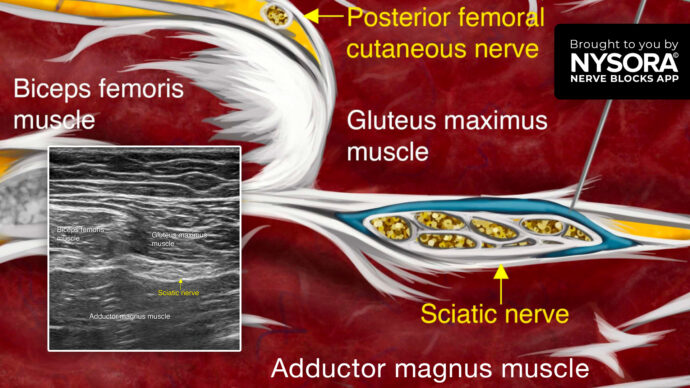
- Place the transducer transversely 3-5 cm above the popliteal fossa between the biceps femoris, and semimembranosus and semitendinosus tendons.
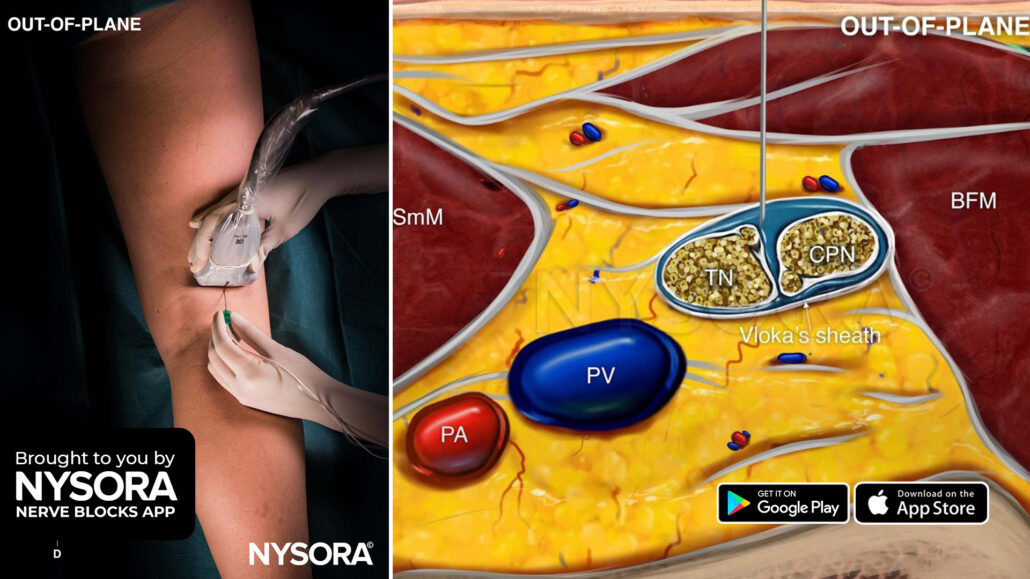
- Identify the sciatic nerve on ultrasound where the tibial (TN) and common peroneal (CPN) nerves start separating but are still within Vloka’s sheath.
- Insert the needle in-plane or out-of-plane into Vloka’s sheath between the TN and CPN, and inject 10-20 mL of local anesthetic.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!