Tips for a Cervical Plexus Block
A cervical plexus block is indicated for carotid endarterectomy, superficial neck procedures, and clavicle fracture analgesia. This block targets the cervical plexus, which is formed by the anterior rami of the C1-C4 cervical spinal nerves. The technique aims to distribute local anesthetic around the plexus’s superficial branches, achieving sensory anesthesia in the anterolateral neck, retro-auricular areas, and the skin above and below the clavicle.
Step-by-step: Three key steps for performing a cervical plexus block
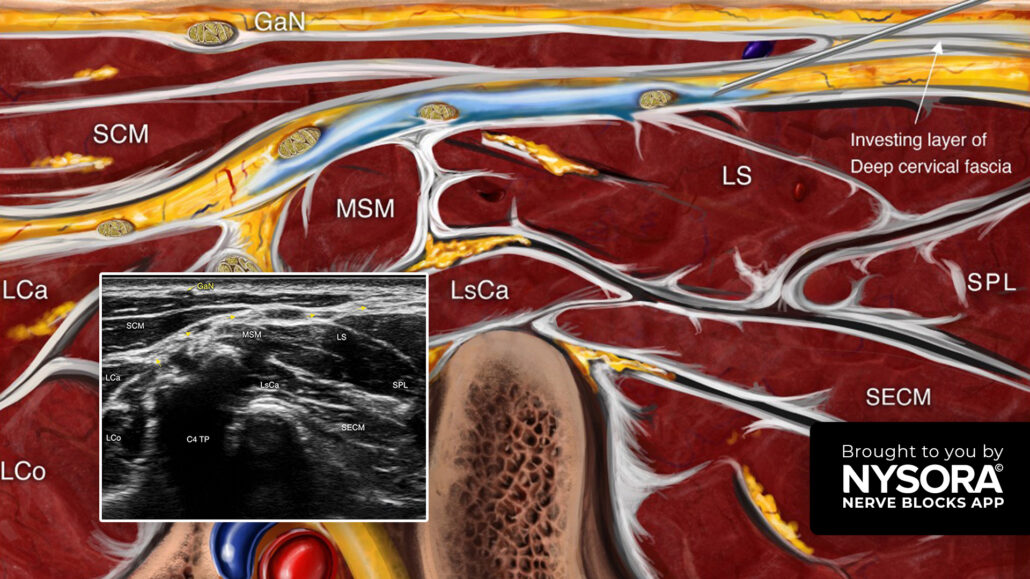
- Place the transducer transversely over the lateral aspect of the neck to identify the sternocleidomastoid muscle (SCM).
- The superficial branches of the cervical branches are located under the SCM.
- Insert the needle in-plane, behind the posterior border of the SCM, and inject 5-8 mL of local anesthetic between the fascial layers containing the branches of the cervical plexus.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!