Nerve Block Tip of the Week: Tibial Nerve Block at the Level of the Ankle
When it comes to foot anesthesia, it’s impossible to construct nerve block techniques to match the osteotomes, myotomes, and dermatomes for each individual surgical procedure. What you do need to know however is which block to use for specific surgical procedures.
An ankle block is indicated for distal foot and toe surgery and anesthetizes the distal ⅓ of the foot. A tibial nerve block at the level of the ankle results in a sensory block of the heel and sole of the foot, and a motor block of plantar flexion of the toes.
We wanted to share these 3 tips to successfully perform a tibial nerve block at the level of the ankle:
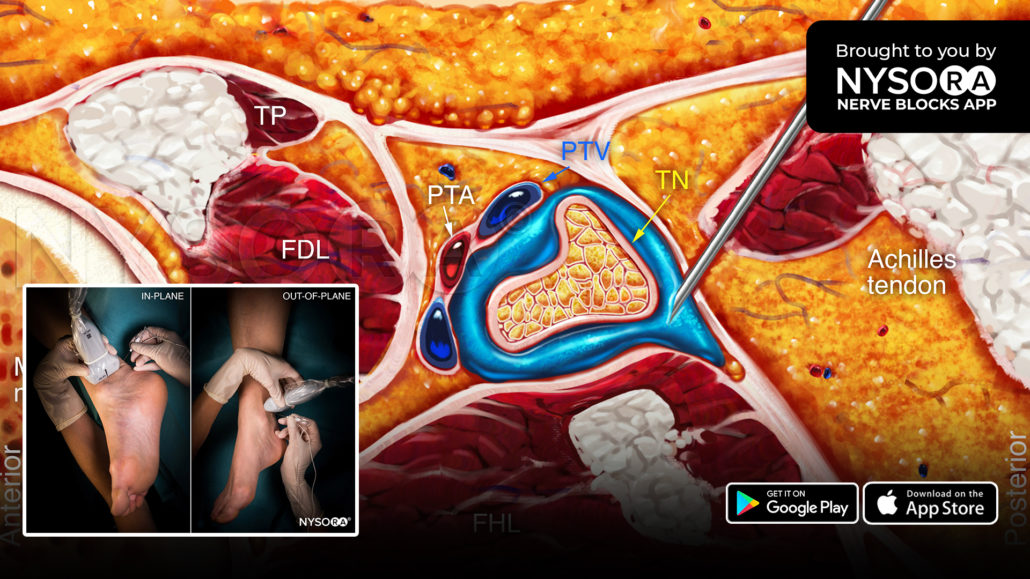
- Place the transducer transversely between the medial malleolus and Achilles tendon.
- Identify the tibial nerve as an oval hyperechoic structure next to the posterior tibial artery and veins, deep to the flexor retinaculum.
- Insert the needle in-plane or out-of-plane to inject 5-8 mL of local anesthetic into the fascial plane enveloping the tibial nerve.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more learning materials on tibial nerve block and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE.