Learning objectives
- Describe the mechanisms of LAST
- Recognize the symptoms of LAST
- Manage LAST occurrence
Definition
- Local anesthetic systemic toxicity (LAST) is a life-threatening adverse event that may occur after the administration of local anesthetics through a variety of routes
- A supratherapeutic plasma concentration of local anesthetics has several adverse effects on the central nervous and cardiovascular systems
Mechanisms of LAST
 Suspected LAST?
Suspected LAST?
Open treatment steps and lipid dosing instantly in the NYSORA Anesthesia Assistant App.
Symptoms
- Central nervous symptoms precede cardiovascular symptoms
- Neurological signs/symptoms range between excitation (early) and depression (late)
- Early LAST: Excitatory manifestations
- Neurological symptoms: Seizures (70%), agitation (10%), loss of consciousness (7%)
- Prodromal (early) symptoms: Perioral paresthesia, metallic taste, tinnitus
- ± 40% of cases present as a sudden, rapid-onset seizure, progressing to cardiac arrest
- High dose of LA or inadvertent IV injection: Prodromal (early) central nervous symptoms may be absent and the first manifestation could be cardiovascular toxicity (11%)
- Cardiovascular toxicity: Heart conduction anomalies, decreased cardiac contractility, decreased systemic vascular resistance
- Early-onset ECG changes: Increased PR and QTc, QRS abnormalities (bundle branch blocks), and increased ST intervals with/without refractory brady-/tachyarrhythmias
- Depression of spontaneous pacemaker activity can rapidly lead to high-degree AV blocks or asystole
- Cardiogenic shock and refractory hypotension may follow as a result of decreased cardiac contractility and vasomotor control disturbances, caused by peripheral vascular ion-channel alterations
Keep in mind
- LAST can occur immediately at the time of injection (usually accidental intravascular injection) or up to an hour after it (due to delayed tissue absorption)
- Continue monitoring for 30-45 min after injection of large volumes or toxic doses of LAs
- Monitor patients with any signs of LAST for 2-6 hrs because cardiovascular depression due to LAs can persist or recur after treatment
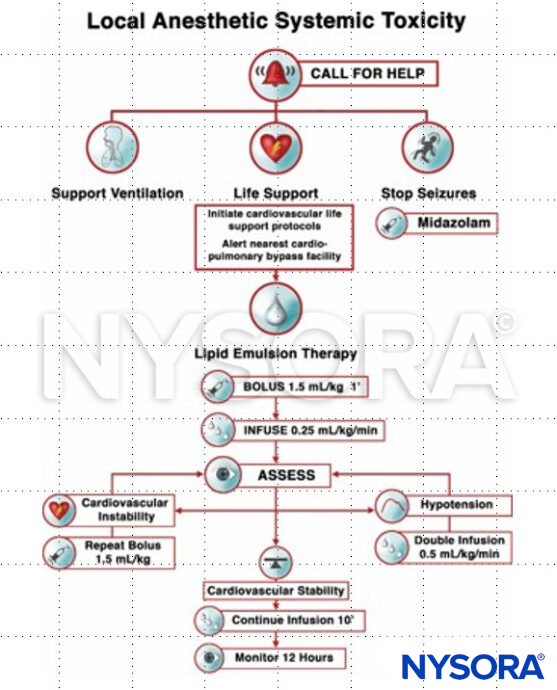
Management
Clinical updates
Bailey et al. (Canadian Journal of Anesthesia, 2025) review pharmacokinetic data for high-volume fascial plane blocks and show that while mean plasma concentrations of ropivacaine, levobupivacaine, and bupivacaine are usually below toxic thresholds, a consistent minority of patients exceed accepted toxicity levels—often without overt LAST symptoms. The review highlights that fixed-volume dosing, higher concentrations, bilateral or continuous infusions, and patient risk factors (pregnancy, extremes of age, cardiac/hepatic disease) substantially increase risk, particularly for TAP, QLB, ESP, and PECS blocks. The authors recommend weight-based (lean body weight) dose calculation, reducing concentration as volume increases, incremental injection with aspiration, close post-block monitoring, and routine consideration of low-dose epinephrine to blunt peak plasma levels.
Shalaby et al. (Clinical and Experimental Emergency Medicine, 2024) focus on “atypical” and delayed presentations of LAST, noting that up to half of cases may lack classic CNS excitation and that simple tissue infiltration accounts for a substantial proportion of events. The authors emphasize routine cardiorespiratory monitoring after local anesthetic administration, strict adherence to the incremental injection protocol with ultrasound guidance, and early initiation of lipid emulsion in accordance with ASRA guidelines. Risk mitigation in the ED should integrate patient selection, dose minimization, and readiness for modified ACLS and ECMO consultation in cases refractory to standard management.
Long et al. (American Journal of Emergency Medicine, 2022) emphasize that LAST, though rare in the emergency department, remains potentially fatal and frequently presents first with neurologic symptoms before cardiovascular collapse. They highlight that inadvertent intravascular injection, high cumulative dosing, and patient factors (extremes of age, cardiac, hepatic, or renal disease, pregnancy) are major contributors, and that bupivacaine carries the greatest cardiotoxic risk. Early recognition, supportive care, and prompt administration of 20% intravenous lipid emulsion are reinforced as the cornerstones of ED management.
Macfarlane et al. (Anaesthesia, 2021) report that the epidemiology of local anesthetic systemic toxicity (LAST) is shifting, with delayed onset increasingly common, a growing proportion of cases arising from fascial plane and field blocks, and more events occurring outside the operating room and involving non-anesthesiologists. Lidocaine now accounts for the majority of reported cases, often related to infiltration or intravenous infusions, while ultrasound guidance has reduced but not eliminated risk. The review reinforces early lipid emulsion therapy, modified resuscitation strategies (low-dose epinephrine, avoidance of vasopressin), and heightened vigilance in high-risk populations.