Nerve Block Tip of the Week: Anterior TAP Block
November 15, 2022
In today’s installment of the Nerve Block Tip of the Week, we are reviewing the Anterior Transversus Abdominis Plane (TAP) Block technique.
The ultrasound-based technique improves the success rate of the anterior TAP block compared to the landmark-based approach as it enables visualization of needle insertion and local anesthetic spread.
Here are 3 tips to further increase the success rate when performing the anterior TAP block.
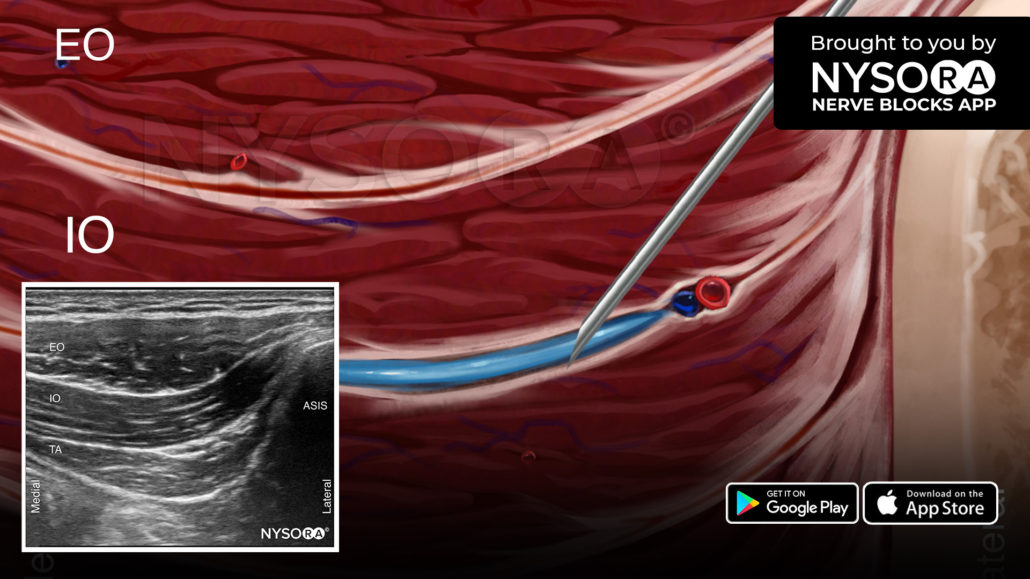
- Place the transducer in an oblique orientation with the lateral edge on top of the anterior superior iliac spine and the medial edge pointing toward the umbilicus.
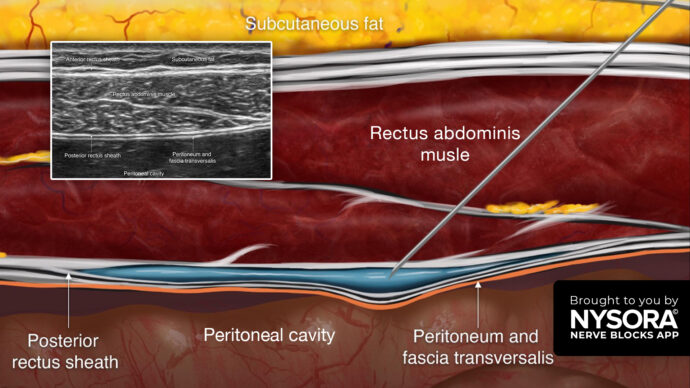
- Identify the three muscle layers of the anterior abdominal wall: External oblique, internal oblique, and transversus abdominis muscles.
- Insert the needle, from lateral to medial, and advance the needle tip until it is placed between the internal oblique and transversus abdominis muscles to inject 15-20 mL of local anesthetic.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips on the Anterior Transversus Abdominis Plane (TAP) Block, as well as the complete guide to the 60 most used nerve blocks, download the Nerve Blocks App HERE.