
Explore NYSORA knowledge base for free:
Explore NYSORA knowledge base for free:


Get yours now and be on the cutting edge of regional anesthesia!
This app is ideal for anesthesiology and pain professionals seeking a comprehensive, on-the-go knowledge base for ultrasound-guided nerve blocks and fascial plane blocks.

Download the NYSORA Nerve Blocks app today and test drive the free blocks!
Cervical plexus block
Sub-Tenon’s (episcleral) eye block
Retrobulbar eye block
Peribulbar eye block
Interscalene brachial plexus block
Supraclavicular brachial plexus block
Infraclavicular brachial plexus block
Costoclavicular brachial plexus
Shoulder block
Axillary brachial plexus block
Nerve blocks above the elbow
Wrist block
Fascia iliaca block – infrainguinal approach
Fascia iliaca block – suprainguinal approach
Hip (PENG) block
Femoral nerve block
Adductor canal block (saphenous nerve)
Lateral femoral cutaneous nerve block
Obturator nerve block
Proximal sciatic nerve block
Popliteal sciatic nerve block
Genicular nerve block
IPACK block
Ankle block
Intercostal nerve block
Pectoralis and serratus plane blocks
Paravertebral block
Transversus abdominis plane
(TAP) blocks
Quadratus lumborum (QL) blocks
Erector spinae plane (ESP) block
Rectus sheath block
A paravertebral block is recommended for pain management following breast surgery, thoracotomy, rib fractures, and procedures involving the thoracic and upper abdominal regions. This technique involves injecting local anesthetic alongside the thoracic vertebra, near where the spinal nerves emerge from the intervertebral foramen. Here are our 3 go-to tips to perform a paravertebral block with the transducer placed in a transverse oblique orientation Place the transducer just lateral to the spinous process at the targeted level in a transverse oblique orientation parallel to the course of the ribs. Visualize the transverse processes and ribs as hyperechoic structures with acoustic shadowing below them. Move the transducer slightly caudad into the intercostal space to identify the tip of the transverse process and the hyperechoic line of the pleura. The hyperechoic internal intercostal membrane can be visualized limiting the thoracic paravertebral space and the adjoining intercostal space as a wedge-shaped hypoechoic layer. Insert the needle in-plane, from lateral to medial, toward the paravertebral space. The goal is to inject the local anesthetic below the internal intercostal ligament, resulting in a downward displacement of the pleura, indicating the proper spread of the local anesthetic. Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life: For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!
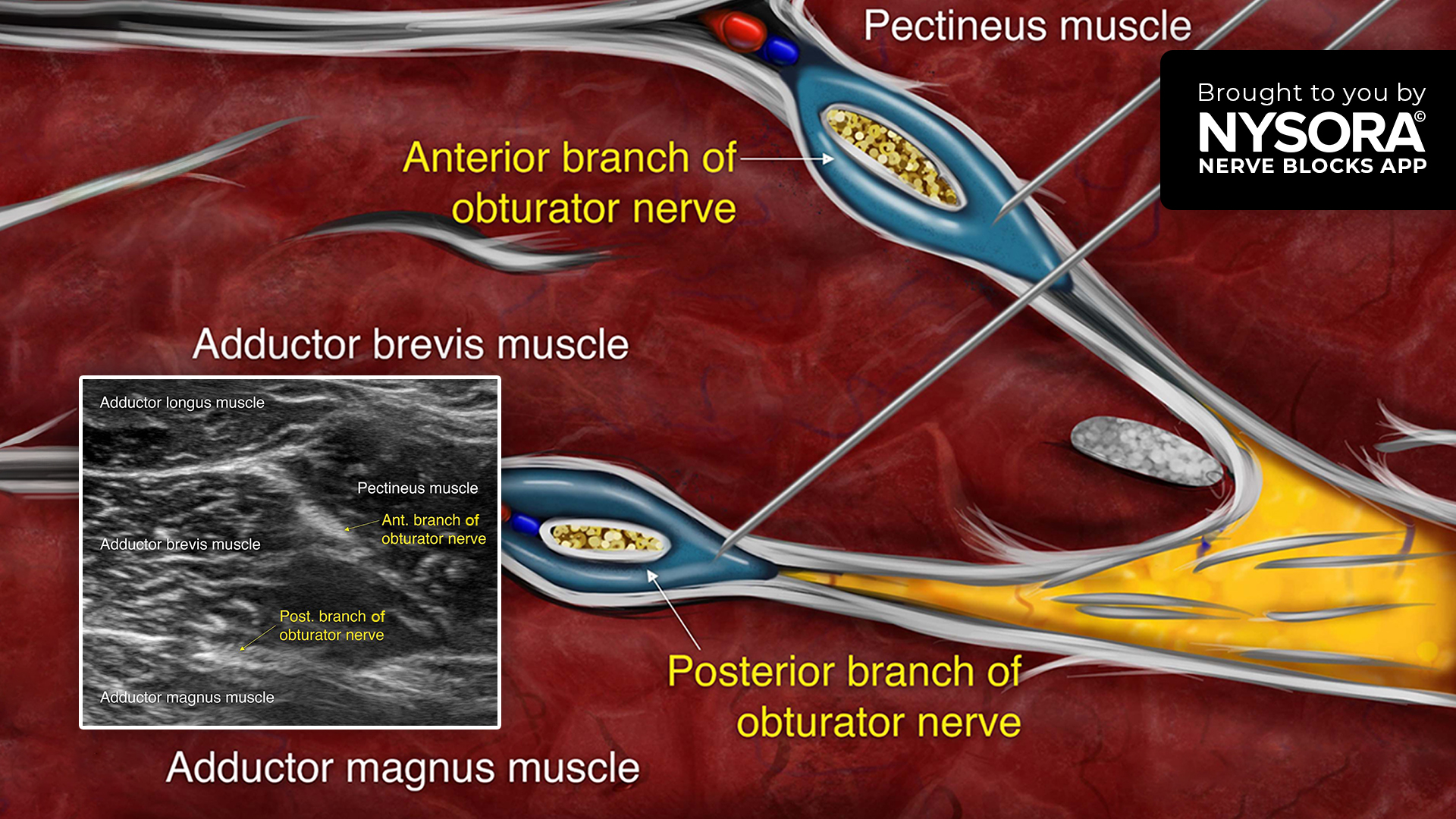
The obturator nerve originates from the ventral rami of the L2 to L4 lumbar nerves. An obturator nerve block serves various purposes: providing supplemental analgesia for hip and knee surgeries, preventing thigh adduction response during transurethral bladder surgery, and relieving painful or permanent hip adductor spasticity. Follow these 3 steps for an obturator nerve block using the distal approach Place the transducer in a transverse orientation perpendicular to the inguinal crease to identify the femoral vessels. Move the transducer medially along the crease to identify the pectineus, and further medially, the adductor longus, brevis, and magnus muscles. The anterior and posterior branches of the obturator nerve can be seen running along the fascial planes superficial and deep to the adductor brevis muscle. Insert the needle in-plane or out-of-plane. Inject two aliquots of local anesthetic into the fascial planes between the adductor longus and adductor brevis muscles (anterior branch) and between the adductor brevis and adductor magnus muscles (posterior branch). Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life: For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!
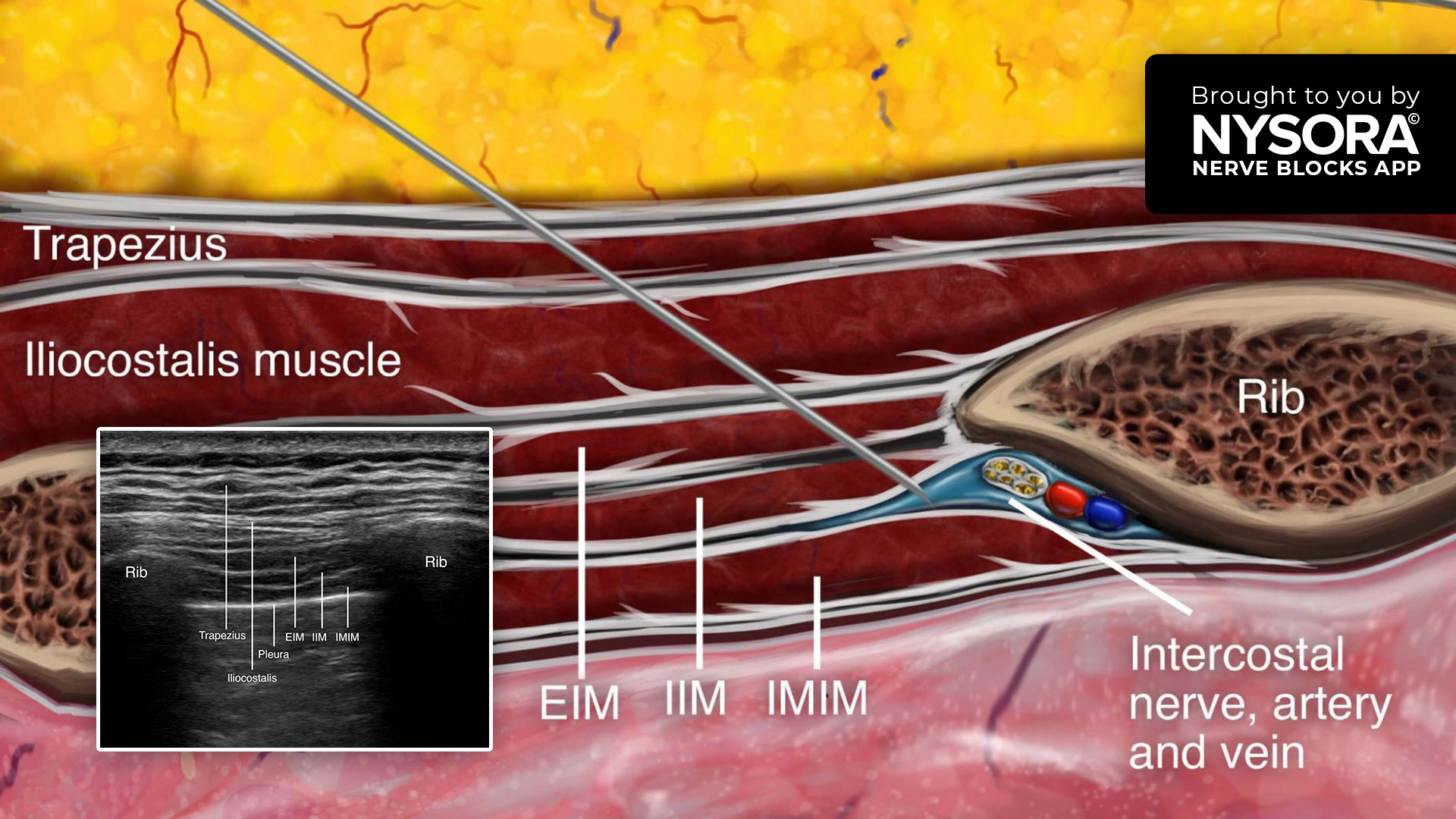
Case presentation A 48-year-old male patient presented with severe pain localized to the left thoracic region, consistent with post-herpetic neuralgia following a recent episode of shingles involving the left T6 dermatome. The patient had no other significant medical history. The pain was described as sharp, burning, and significantly impacting the patient’s daily activities. Conventional analgesic medications provided limited relief, prompting the consideration of an ultrasound-guided intercostal nerve block for targeted pain management. Nerve block technique A high-frequency linear transducer was used to scan the left thoracic region, focusing on the intercostal spaces. Real-time ultrasound imaging provided identification of the targeted intercostal space, ribs, and underlying neurovascular structures. Intercostal nerve block; transducer position and sonoanatomy. IMIM, innermost intercostal muscle; IIM, internal intercostal muscle; EIM, external intercostal muscle. Next, a 25-gauge needle was inserted in-plane to penetrate the external and internal intercostal muscles. The optimal target needle endpoint is the location just below the internal intercostal muscle to ensure that the needle tip remains superficial to the parietal pleura. Then, 4 mL of bupivacaine 0.5% with 1:300,000 epinephrine was injected into the intercostal sulcus around the intercostal nerve. The procedure was repeated for additional intercostal spaces, depending on the extent of the patient’s pain and response. Intercostal nerve block; Reverse Ultrasound Anatomy with needle insertion in-plane and local anesthetic spread (blue). IMIM, innermost intercostal muscle; IIM, internal intercostal muscle; EIM, external intercostal muscle. Patient outcome Following the ultrasound-guided intercostal nerve block, the patient experienced significant pain relief within 30 minutes. The sharp, burning pain was reduced to a mild ache, allowing him to resume normal activities. Over the next few days, the pain continued to diminish, and the patient reported improved sleep and overall functionality. No adverse events or complications were observed. For more case studies like these and the complete guide […]
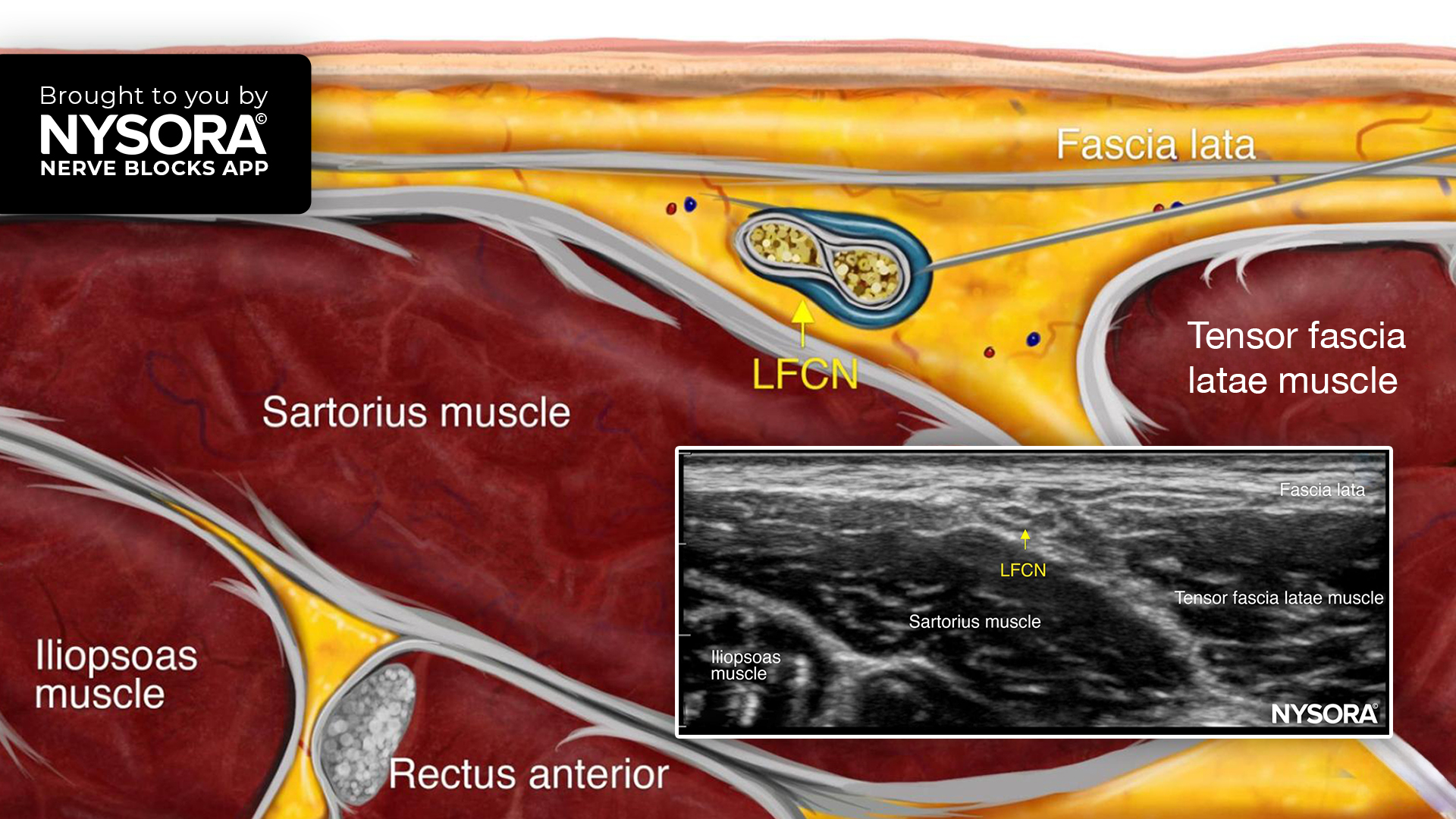
The lateral femoral cutaneous nerve (LFCN) block is indicated for analgesia for surgery on the anterolateral thigh (e.g., skin grafting), muscle biopsy, and meralgia paresthetica. The complex branching of the LFCN makes accurate landmark-based blocks difficult, but ultrasound guidance ensures precise needle placement, enhancing pain relief and outcomes. Here are our 3 go-to tips for performing an LFCN block Place the transducer in a transverse position just distal to the anterior superior iliac spine (ASIS) to identify the sartorius muscle. Identify the LFCN as a hyperechoic structure moving superficially to the muscle toward a tiny space between the sartorius and tensor fascia latae muscles. Insert the needle in-plane or out-of-plane deep to the fascia lata next to the nerve and inject 3-5 mL of local anesthetic. Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life: For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!

Case presentation A 69-year-old patient, 156 cm tall, weighing 90 kg, with a long history of diabetes mellitus, presented with foot gangrene and was scheduled for wound debridement and potential amputation. The patient’s hemodynamic status was stable, and no signs of systemic infection were observed. Relevant medications included insulin and low-molecular-weight heparin, which had been discontinued 48 hours prior to the procedure. Airway assessment indicated Mallampati Class 2 (MP 2). Anesthesia plan The patient’s hemodynamic stability and absence of systemic infection allowed for the consideration of general anesthesia. However, postoperative pain management posed a challenge due to the potential need for opioids and associated risks. To mitigate these risks, the utilization of peripheral nerve blocks was explored as an alternative approach. Specifically, a popliteal block with 20 mL ropivacaine 0.5% and a femoral triangle block for saphenous nerve territory coverage using 5 mL of ropivacaine 0.5% were performed, allowing for effective pain management and avoiding airway instrumentation, intubation, and mechanical ventilation. Patient outcome The combination of the popliteal block and femoral triangle block resulted in complete pain management for 24+ hours. By utilizing nerve blocks, prolonged pain relief can be achieved, reducing the reliance on systemic opioids and lowering associated risks. Explore additional case studies and access the comprehensive guide to the 60 most common nerve blocks by downloading the Nerve Blocks App HERE. Don’t pass up the opportunity to acquire the bestselling NYSORA Nerve Blocks App, now also available in book format – the ideal study companion to complement the app!
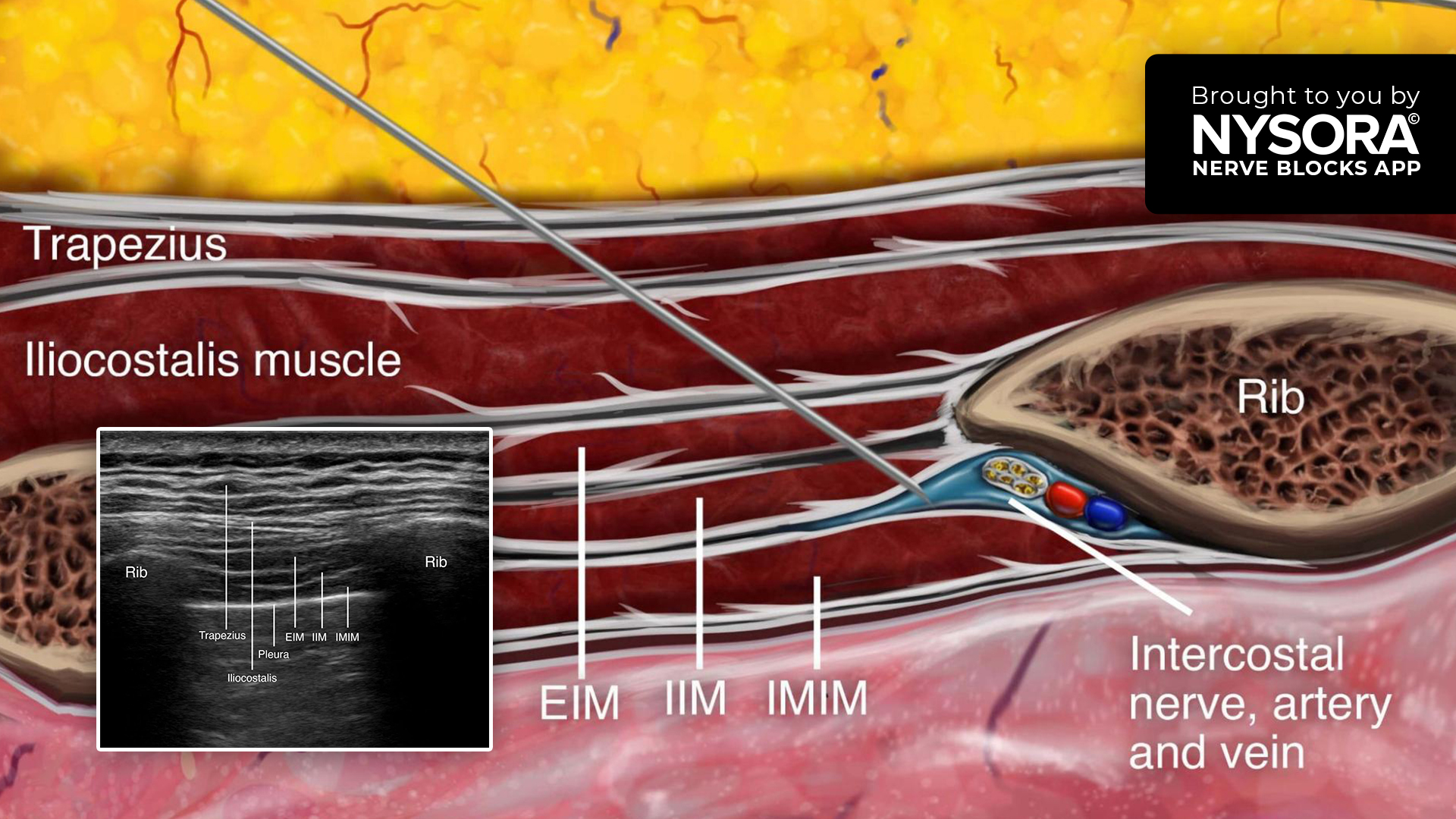
An intercostal nerve block provides analgesia for rib fractures, postsurgical analgesia for chest and upper abdominal surgery (e.g., thoracotomy, thoracostomy, mastectomy, gastrostomy, and cholecystectomy), herpes zoster, or post-herpetic neuralgia. Here are the 4 steps we follow to perform an intercostal nerve block Place the transducer lateral to the angle of the rib in a sagittal oblique orientation perpendicular to the direction of two palpable ribs. Continue by scanning the intercostal space laterally between the costal angle and posterior axillary line where the neurovascular bundle has not yet divided. Insert the needle in-plane or out-of-plane to penetrate the external and internal intercostal muscles. The optimal target needle endpoint is the location just below the internal intercostal muscle to ensure that the needle tip remains superficial to the parietal pleura. Complete the block with 3-5 mL of local anesthetic at each level. Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life: For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!

Case presentation A 45-year-old female patient with a confirmed diagnosis of carpal tunnel syndrome in the right hand was scheduled for elective carpal tunnel release surgery. The patient experienced significant pain, numbness, and tingling in the affected hand, affecting daily activities and quality of life. As part of the comprehensive pain management plan, an ultrasound-guided wrist block was proposed to provide localized anesthesia and minimize postoperative pain. Nerve block technique The wrist block technique consists of a mid-forearm level block of the median and ulnar nerves, followed by a subcutaneous infiltration of the local anesthetic at the wrist crease for any remaining cutaneous branches of the musculocutaneous, radial, or ulnar nerves. Subcutaneous infiltration. Under ultrasound guidance, the median and ulnar nerves were identified between the superficial and deep flexors of the wrist and fingers. Median nerve block at the level of the wrist; transducer position and sonoanatomy. MN, median nerve; FPL, flexor pollicis longus muscle; FDS, flexor digitorum superficialis muscle; FDP, flexor digitorum profundus muscle. Ulnar nerve block at the level of the wrist; transducer position and sonoanatomy. UN, ulnar nerve; UA, ulnar artery; FCU, flexor carpi ulnaris; FDP, flexor digitorum profundus muscle; FDS, flexor digitorum superficialis muscle. A 25-gauge needle was then inserted in-plane or out-of-plane and 4 mL of lidocaine 2% was injected into the fascia containing the nerves. The onset of anesthesia was observed within 10 minutes. Median nerve block at the level of the wrist; Reverse Ultrasound Anatomy with needle insertion out-of-plane and local anesthetic spread (blue). MN, median nerve; FPL, flexor pollicis longus muscle; FDS, flexor digitorum superficialis muscle; FDP, flexor digitorum profundus muscle. Ulnar nerve block at the level of the wrist; Reverse Ultrasound Anatomy with needle insertion in-plane and local anesthetic spread (blue). UN, ulnar nerve; UA, ulnar artery; FCU, flexor carpi ulnaris; […]
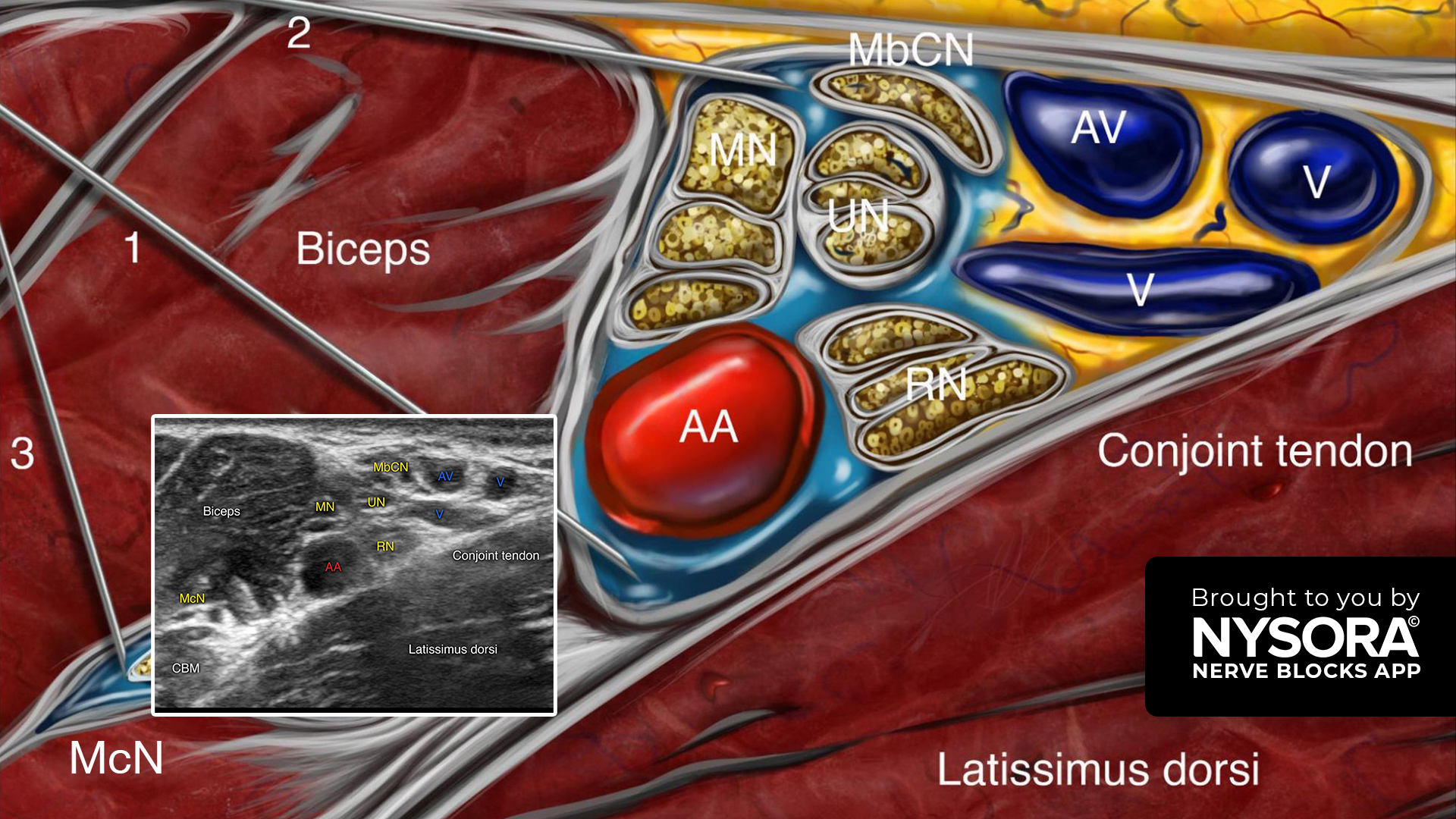
The most common indications for an axillary brachial plexus block include surgery of the forearm, wrist, or hand of moderate to long duration, with or without an arm tourniquet. It anesthetizes the brachial plexus at the level of the terminal branches (i.e., median, ulnar, radial, and musculocutaneous nerves), resulting in anesthesia of the upper extremity from the mid-arm down, including the hand. Step-by-step: 3 key steps for performing an axillary brachial plexus block Place the transducer in a transverse orientation over the intersection of the pectoral major and biceps muscle insertion. Do not place the transducer too high in the axillary fossa. Identify the axillary artery, the conjoint tendon, the neurovascular sheath containing the median, ulnar, and radial nerves, the muscles (i.e., biceps, coracobrachialis, and latissimus dorsi muscles), and the musculocutaneous nerve. Insert the needle in-plane, from lateral to medial, toward the axillary artery and inject 20 mL of local anesthetic (8 mL above the axillary artery, 8 mL below the axillary artery, and 4 mL for the musculocutaneous nerve). Tip: When the musculocutaneous nerve travels together with the median nerve, it is not necessary to block this nerve with a separate injection. Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life: For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!
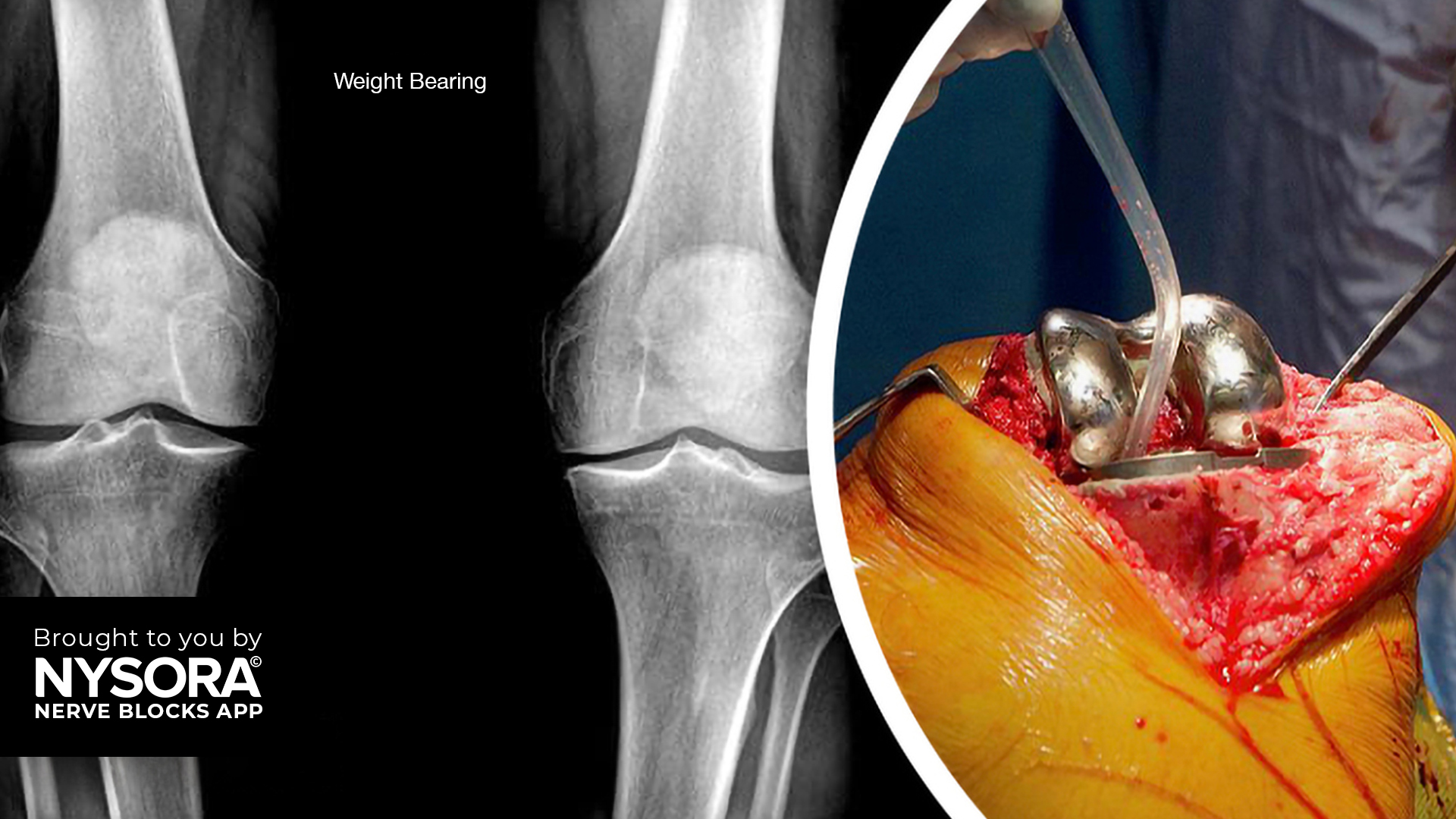
Case presentation A 65-year-old male patient with severe osteoarthritis of the right knee was scheduled for elective total knee arthroplasty. The patient had a history of chronic knee pain and limited mobility and was keen on exploring options for effective pain relief. As part of the comprehensive pain management plan, an ultrasound-guided femoral nerve block was planned to provide targeted analgesia for improved pain control. Nerve block technique The patient was positioned supine with the lower extremity fully extended and slightly rotated externally. A high-frequency linear transducer was placed in a transverse orientation over the femoral crease to identify the femoral nerve. Femoral nerve block; transducer position and sonoanatomy. FA, femoral artery; FV, femoral vein; FN, femoral nerve. A 22-gauge needle was inserted in-plane, in a lateral-to-medial direction, to pierce the fascia iliaca lateral to the femoral nerve. A total of 12 mL of bupivacaine 0.5% was injected ensuring proper spread around the femoral nerve. Femoral nerve block; Reverse Ultrasound Anatomy with needle insertion in-plane and local anesthetic spread (blue). FA, femoral artery; FV, femoral vein; FN, femoral nerve. Patient outcome Following the ultrasound-guided femoral nerve block, the patient experienced significant pain relief within minutes. The patient reported improved comfort, allowing for early mobilization and participation in physical therapy. The need for systemic opioids was greatly reduced, thereby minimizing associated side effects such as sedation and nausea. The patient did not experience any immediate or delayed complications related to the nerve block. For more case studies like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!
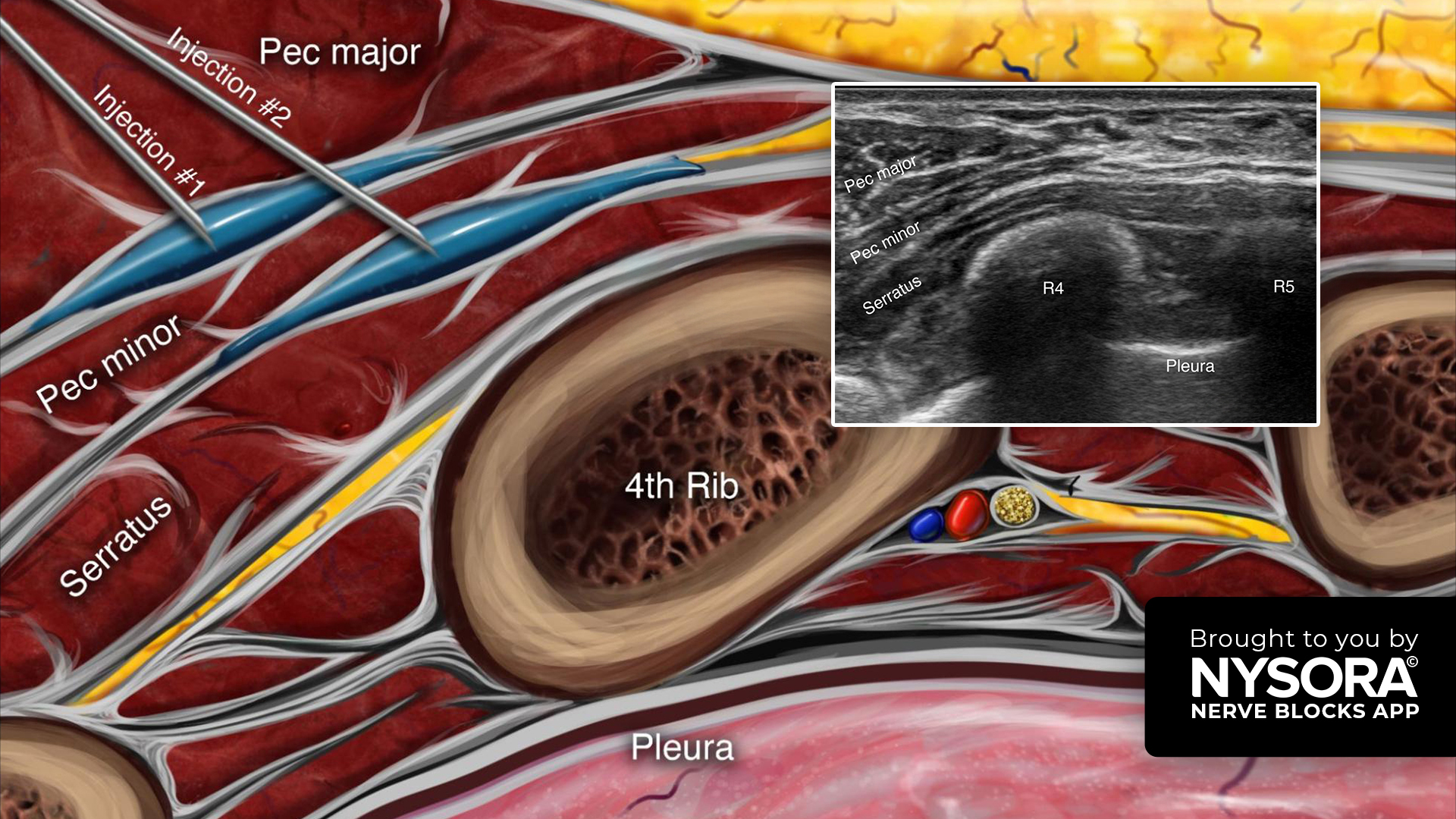
The PEC II block anesthetizes the lateral and medial pectoral nerves, the anterior lateral cutaneous branches of the intercostal nerves, and the intercostobrachialis, providing analgesia for extensive breast surgery, thoracic wall procedures, and sentinel node excision. Here are our 3 go-to tips to perform a PEC II block Place the transducer in a sagittal orientation below the midline of the clavicle. From the PEC I position, slide the transducer laterally to identify the 4th and 5th ribs and the serratus anterior muscle. Insert the needle in-plane, from anterior to posterior, through the pectoralis major muscle and inject local anesthetic in two fascial planes. – 10 mL between the pectoralis major and minor muscles (PEC I). – 15-20 mL between the pectoralis major and serratus anterior muscles (PEC II). Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life: For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!
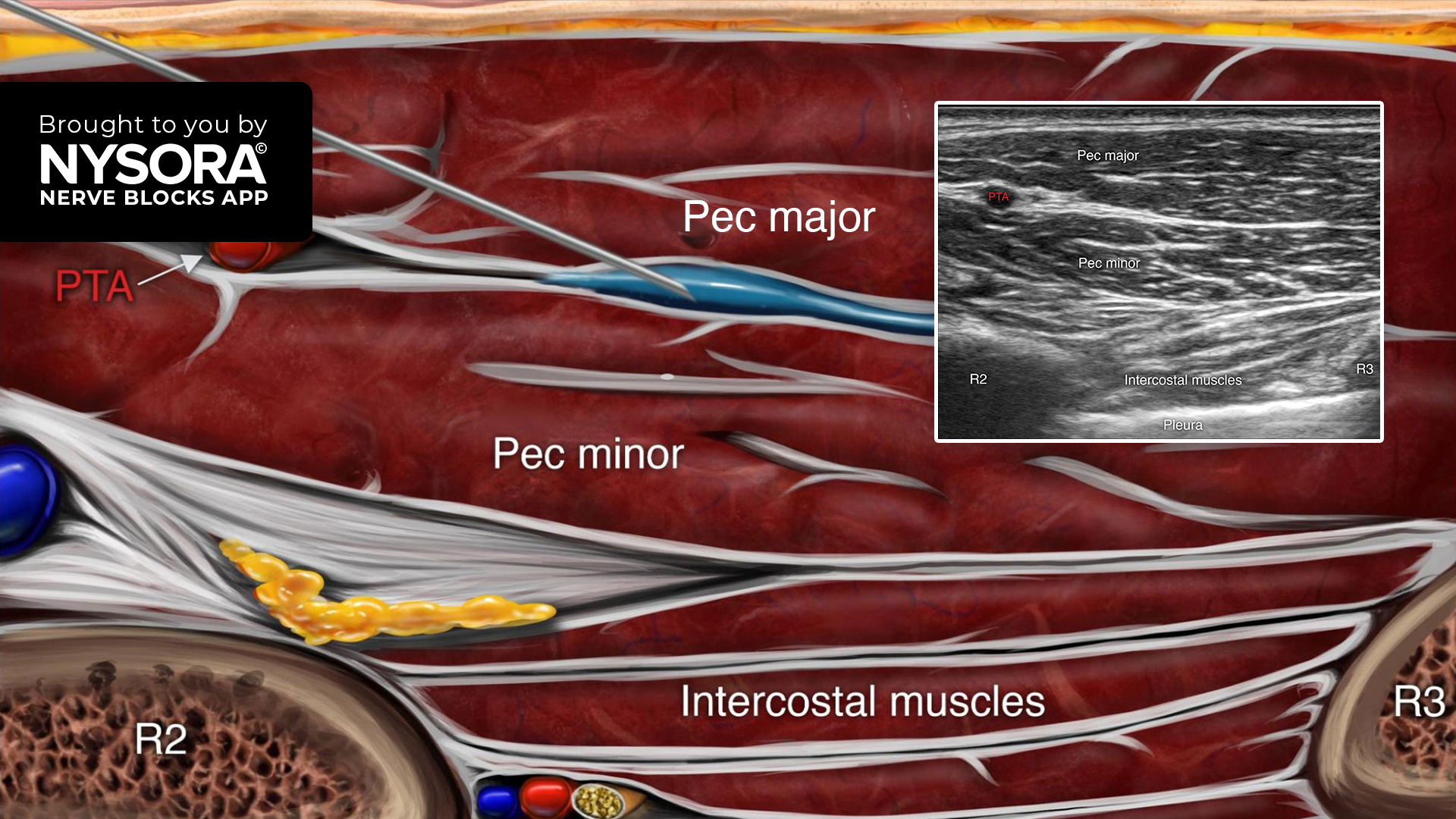
The PEC I block, targeting the medial and lateral pectoral nerves that supply the pectoralis muscles, is used to provide analgesia for surgeries involving the breast, clavicle, and acromioclavicular joint. It is particularly indicated for procedures involving the pectoralis major muscle, including breast prosthesis insertion, implantable cardiac device placement, and anterior thoracotomies. Learn the 3 key steps to successfully perform a PEC I block: Place the transducer in a sagittal orientation below the midline of the clavicle. Identify the pectoralis major and minor muscles with the axillary artery, vein, and elements of the brachial plexus lying under the fascia of the pectoralis minor. Slide the transducer caudally to identify the 2nd and 3rd ribs. Insert the needle in-plane, from cephalad to caudal, and inject 10-20 mL of local anesthetic between the pectoralis major and minor muscles. Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life: For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!

Case presentation A 70-year-old patient with a history of renal insufficiency presented at our facility with a bimalleolar fracture. The patient was scheduled for the removal of an external fixator, followed by open reduction and internal fixation (ORIF) in the prone position. Importantly, the patient expressed a preference to avoid general anesthesia. Anesthesia plan Given the patient’s preference and medical history, the anesthesia team opted for a combination of spinal anesthesia and a peripheral nerve block. Initially, spinal anesthesia was administered using 10 mg (2 mL) of isobaric bupivacaine 0.5%. Subsequently, once the patient was positioned prone in the operating room, a popliteal block was performed using 15 mL of ropivacaine 0.5%. This approach was chosen to provide both intraoperative anesthesia and postoperative pain relief. A tourniquet was placed above the knee to facilitate the surgical procedure. Reverse Ultrasound Anatomy for a popliteal block with needle insertion out-of-plane. The local anesthetic spread is shown in blue. TN, tibial nerve; CPN, common peroneal nerve; PA, popliteal artery; PV; popliteal vein; SmM, semimembranosus muscle; BFM, biceps femoris muscle. Patient outcome The combination of spinal anesthesia and popliteal block was successful in providing adequate anesthesia for the duration of the surgery. The patient reported minimal discomfort and remained hemodynamically stable throughout the procedure. Postoperatively, the patient experienced effective pain relief from the popliteal block. This case highlights the effectiveness of combining spinal anesthesia with a peripheral nerve block in patients where general anesthesia is either contraindicated or not preferred. It also demonstrates the importance of individualizing anesthesia plans to cater to patient preferences and specific health conditions. For more case studies like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App […]
Regional anesthesia numbs a specific area of the body, blocking pain in that region during and after surgical procedures. Unlike general anesthesia, which renders the patient unconscious, regional anesthesia allows the patient to remain awake or lightly sedated without feeling pain in the targeted area. This is achieved by inhibiting the transmission of pain signals to the brain.
Regional anesthesia has several benefits, such as minimized systemic opioid requirements, reduced postoperative pain and nausea, and improved recovery rates. It also decreases the risk of complications associated with general anesthesia, making it a preferred choice for specific patient populations and surgical interventions. Additionally, it can provide pain relief for several hours or days after the procedure.
Ultrasound-guided nerve blocks are a medical procedure used to alleviate pain by targeting specific nerves by administering local anesthetics or other therapeutic agents. Ultrasound imaging visualizes the nerves and surrounding structures in real-time, allowing for precise needle placement and injection.
Ultrasound-guided nerve blocks provide numerous advantages. They intensify accuracy and precision by enabling clear visualization of the targeted nerve and surrounding structures, minimizing the likelihood of errors in needle placement. This increases the efficacy of the procedure but also reduces the risk of complications such as inadvertent vascular puncture or nerve damage. Furthermore, the real-time visualization with ultrasound allows for immediate adjustments during needle placement, optimizing the delivery of medication and ensuring its effective localization.
Nerve blocks offer precise pain control in specific regions of the body for surgical procedures, trauma management, and pain interventions. By delivering anesthesia directly to the site of action, nerve blocks minimize systemic side effects associated with general anesthesia, improving patient safety and comfort. They can also reduce the need for general anesthesia, leading to shorter hospital stays, decreased opioid consumption, earlier mobilization, and faster recovery times. Moreover, these nerve blocks enhance surgical conditions by providing optimal anesthesia to the surgical site, thereby improving surgical outcomes and patient satisfaction.
The NYSORA Nerve Blocks App is designed to cater to a diverse global audience, ensuring that healthcare professionals worldwide can access its comprehensive educational content on nerve block techniques. As of the latest update, the app is available in multiple languages, including English, Spanish, Portuguese, Chinese, Japanese, French, Dutch, and German. This multilingual support underscores NYSORA's commitment to promoting excellence in regional anesthesia and pain management across different linguistic and cultural backgrounds.
Download the NYSORA Nerve Blocks app today and test drive the free blocks!




Join our mailing list and get weekly educational updates delivered straight to your inbox.