
Explore NYSORA knowledge base for free:
Explore NYSORA knowledge base for free:



Get yours now and be on the cutting edge of regional anesthesia!
This app is ideal for anesthesiology and pain professionals seeking a comprehensive, on-the-go knowledge base for ultrasound-guided nerve blocks and fascial plane blocks.

Download the NYSORA Nerve Blocks app today and test drive the free blocks!
Cervical plexus block
Sub-Tenon’s (episcleral) eye block
Retrobulbar eye block
Peribulbar eye block
Interscalene brachial plexus block
Supraclavicular brachial plexus block
Infraclavicular brachial plexus block
Costoclavicular brachial plexus
Shoulder block
Axillary brachial plexus block
Nerve blocks above the elbow
Wrist block
Fascia iliaca block – infrainguinal approach
Fascia iliaca block – suprainguinal approach
Hip (PENG) block
Femoral nerve block
Adductor canal block (saphenous nerve)
Lateral femoral cutaneous nerve block
Obturator nerve block
Proximal sciatic nerve block
Popliteal sciatic nerve block
Genicular nerve block
IPACK block
Ankle block
Intercostal nerve block
Pectoralis and serratus plane blocks
Paravertebral block
Transversus abdominis plane
(TAP) blocks
Quadratus lumborum (QL) blocks
Erector spinae plane (ESP) block
Rectus sheath block
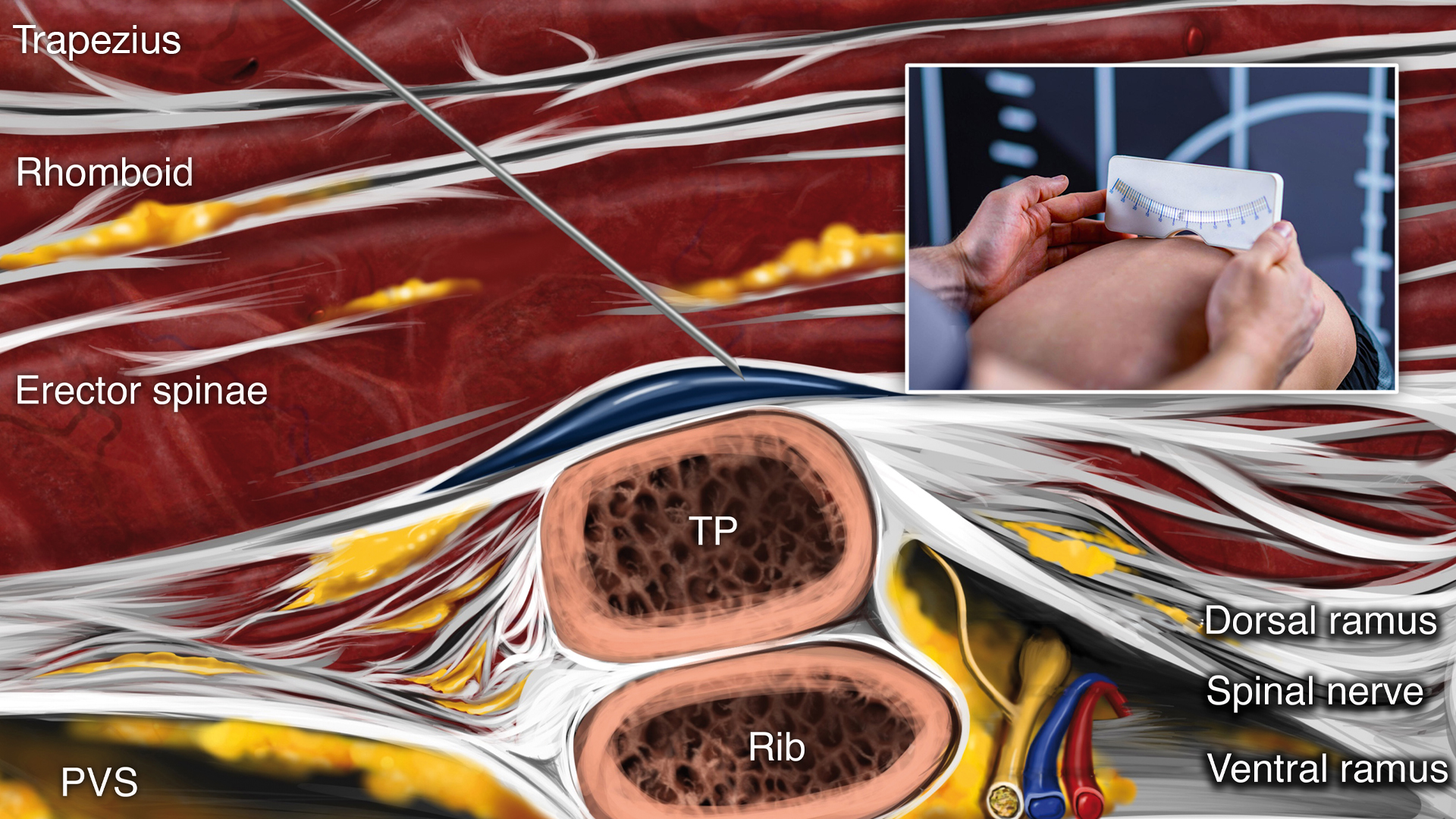
Adolescent idiopathic scoliosis (AIS) is a condition affecting 1-3% of adolescents aged 10-16, characterized by a curvature of the spine with no identifiable cause. For most patients, this condition remains mild and manageable, but in severe cases, surgical intervention through posterior spinal fusion (PSF) becomes necessary. Effective pain management following PSF is crucial to ensuring a smooth recovery and enhancing patient outcomes. Currently, multimodal analgesia, which involves combining various pain relief methods, is the standard approach. However, the role of advanced regional anesthesia techniques, such as the erector spinae plane block (ESPB), remains under-explored in pediatric populations. The ESPB is a novel regional anesthesia technique that involves injecting a local anesthetic near the spine to block pain transmission effectively. This technique has shown promising results in managing pain in adult spine surgeries and some pediatric procedures. However, its use in pediatric patients undergoing PSF for AIS has been limited. This study aimed to evaluate the practicality and effectiveness of integrating ESPB into a rapid recovery pathway for pediatric patients following PSF. Study objective and methods This prospective, randomized controlled trial enrolled 24 patients aged 10-19 years, all of whom were undergoing multilevel PSF for AIS correction. Patients were excluded if they had chronic pain conditions requiring neuromodulating medications, neuromuscular scoliosis, a history of chronic opioid therapy, or allergies/contraindications to the study medications or techniques. Participants were randomly assigned to two groups: one group of 12 patients received bilateral ESPB before the surgical incision, while the other 12 patients served as the control group and did not receive ESPB. ESPBs were administered using ultrasound guidance to inject a mixture of 0.25% bupivacaine and dexamethasone near the T7 vertebrae. Patients were evaluated at multiple time points for pain scores, satisfaction, and opioid consumption (oral morphine equivalents) during their hospital stay. The primary […]
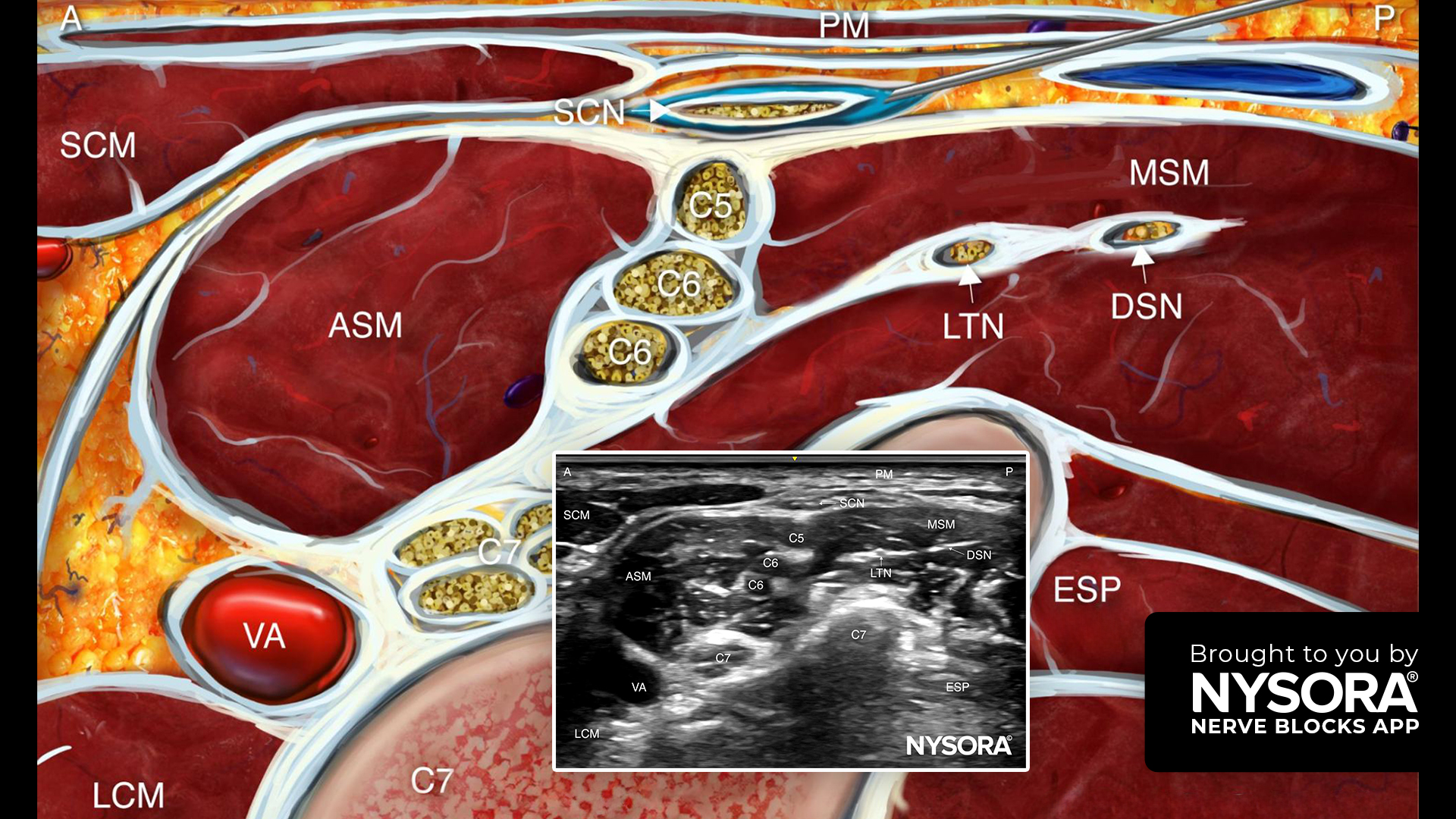
This advanced technique offers targeted analgesia for shoulder surgeries, clavicle operations, and upper anterior thoracic wall procedures, enhancing the effectiveness of brachial plexus and interpectoral plane blocks. Technique overview The supraclavicular nerves selective block is performed at the base of the posterior triangle of the neck, cranial to the clavicle. This technique is indicated for open shoulder surgery (in combination with a brachial plexus block), clavicle surgery, and procedures on the upper anterior thoracic wall, such as the placement of implantable electronic devices or long-term catheters, often in combination with an interpectoral plane block. Key points Goal: Local anesthetic spread around the nerves superficial to the investing layer of the deep cervical fascia Transducer: Linear Needle: 25-gauge, 2.5-4 cm Local anesthetic volume: 1-5 mL Patient position: Supine with the head turned to the contralateral side to maximize exposure of the neck Read more about the Supraclavicular Nerves Selective Block and how it can benefit your patients. Download the NYSORA Nerve Blocks App HERE to access detailed guides, high-resolution images, and expert tips for this and many other nerve block techniques.
Renal transplantation is a critical treatment for end-stage renal disease, but managing postoperative pain remains challenging due to the altered pharmacokinetics in kidney graft recipients. While opioids are commonly used for pain relief, their side effects can complicate recovery. Given the limited non-opioid analgesic options, the anterior quadratus lumborum (QL) block, a relatively new technique, was investigated for its potential to reduce opioid consumption and improve pain management in this context. This study specifically aimed to determine if the unilateral anterior QL block could effectively lower postoperative opioid use following living-donor renal transplantation within a multimodal analgesia framework. Study objective and methods The study was a double-blinded randomized controlled trial involving 88 adult patients undergoing living-donor renal transplantation. Participants were randomly assigned to receive either a unilateral anterior QL block with 30 mL of ropivacaine 0.375% or a sham block with normal saline. All patients received standard multimodal analgesia, including acetaminophen and fentanyl via intravenous patient-controlled analgesia (PCA). The primary outcome measured was total opioid consumption during the first 24 hours post-transplantation. Secondary outcomes included pain scores, time to first opioid administration, cutaneous sensory block, motor weakness, nausea/vomiting, quality of recovery scores, time to first ambulation, and length of hospital stay. Key findings Primary outcome: The total opioid consumption in the first 24 hours post-transplantation did not differ significantly between the QL block group and the control group (median 160.5 mg vs. 187.5 mg oral morphine equivalent; p=0.29). Secondary outcomes: Similarly, no significant differences were observed in pain scores, time to first opioid administration, incidence of nausea/vomiting, or other secondary outcomes. Conclusion The study concluded that the anterior QL block does not reduce postoperative opioid consumption or pain scores in patients receiving multimodal analgesia after living-donor renal transplantation. Therefore, routine use of the anterior QL block in this surgical population […]
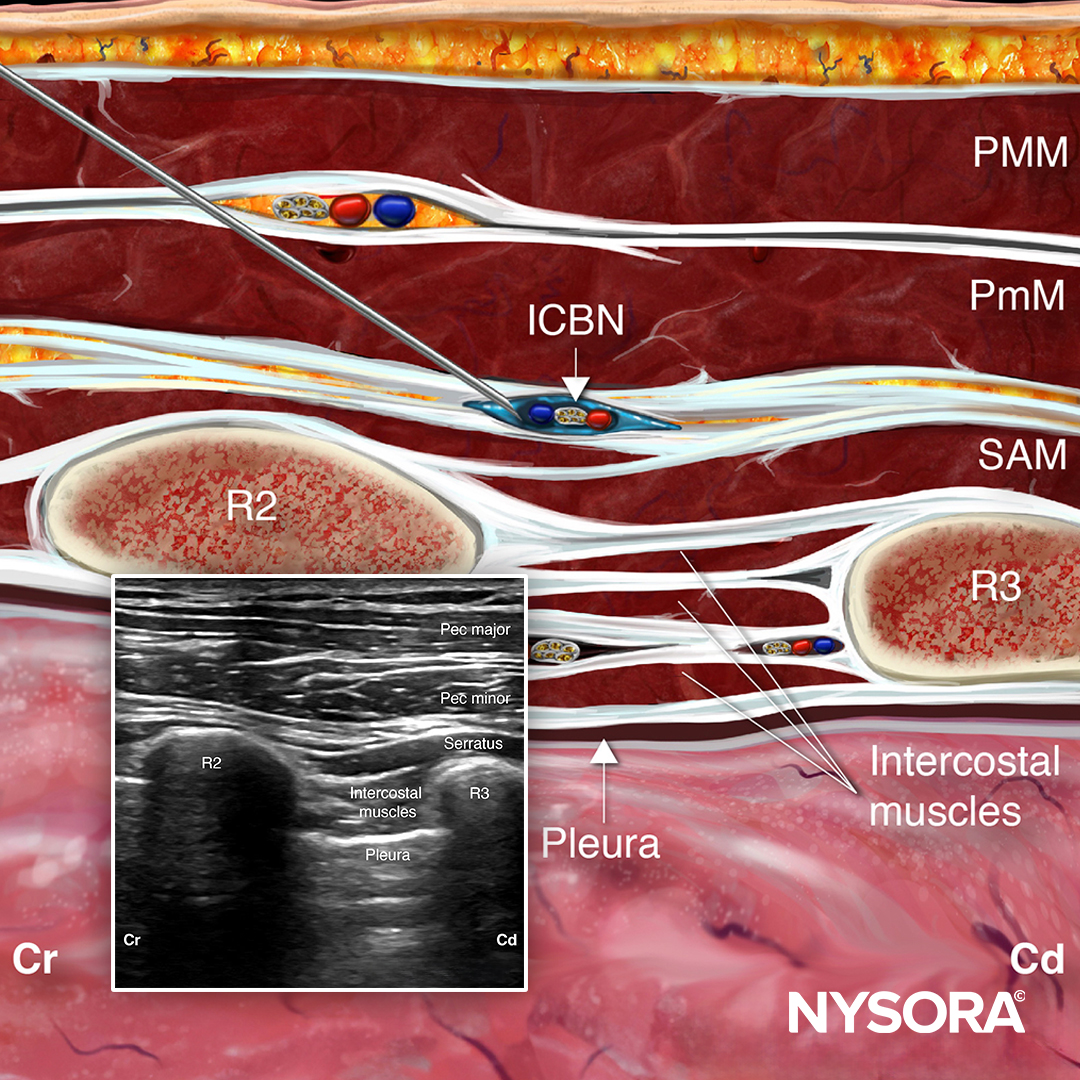
We’re excited to introduce the Intercostobrachial Nerve Block (ICBN) technique to the NYSORA Nerve Blocks App! This advanced technique provides outstanding pain relief for surgeries involving the upper arm and axilla, and has gained popularity as an adjunct to brachial plexus blocks for achieving complete upper extremity anesthesia. Technique overview The ICBN block is performed at the T2 intercostal space or the axilla. It is particularly effective for providing analgesia for surgeries involving the posteromedial aspect of the arm and axillary fossa, such as the superficialization of the basilic vein for brachiobasilic arteriovenous fistula and elbow surgery. Additionally, it is beneficial for managing chronic pain following a mastectomy. This block can be utilized alone or in combination with other regional anesthesia techniques to ensure comprehensive pain control for procedures extending beyond the ICBN distribution. Key points Goal: Local anesthetic spread at the T2-T3 intercostal space at the anterior axillary line or along the conjoint tendon at the axilla Transducer: Linear Needle: 5 cm Local anesthetic volume: 5 mL Patient position: Supine with the head turned to the contralateral side and the arm abducted 90° Discover how the Intercostobrachial Nerve Block can improve patient outcomes. Download the NYSORA Nerve Blocks App HERE to access detailed guides, high-resolution images, and expert tips on these and numerous other nerve block techniques.

For over two decades, NYSORA has been a beacon of excellence in anesthesia education. From our beginnings with educational outreach programs across Asia in the 2010s to our ongoing initiatives in Latin America and beyond, we’ve consistently set the standard for high-quality, accessible medical education. With the advent of social media and internet communication, our reach has expanded even further, allowing us to receive continuous accolades and gratitude for our educational efforts. One of the crowning achievements in our portfolio is the NYSORA Nerve Blocks App, trusted by over 15,000 anesthesia professionals worldwide. What’s New in the NYSORA Nerve Blocks App? We are thrilled to announce that the NYSORA Nerve Blocks App will soon receive a significant update with the 2025 Edition! This update promises to boost your nerve block game and add more value to your practice. Here’s a sneak peek at what’s coming: Expanded Visual Library High-Definition Visuals: Our visual library has been significantly expanded and now includes a wide array of new ultrasound images and illustrations. These visuals meticulously detail the ideal transducer position and needle insertion techniques for various nerve block procedures. Enhanced Learning: Designed to provide a more immersive experience, these images will facilitate a deeper understanding and more precise application of the different nerve block techniques. 3D Patient Position Images New 3D Patient Position Images: We’ve added 3D images to deepen your understanding of patient positioning. These tools allow you to apply techniques with greater confidence and precision, ultimately leading to better patient outcomes in your practice. Detailed Clinical Videos Comprehensive Overview: Our latest update includes newly added clinical videos covering all aspects of the nerve block technique. These videos are packed with essential tips and offer a comprehensive overview, ensuring you’re prepared for any scenario. Hands-On Guidance: Whether you’re a novice or an […]
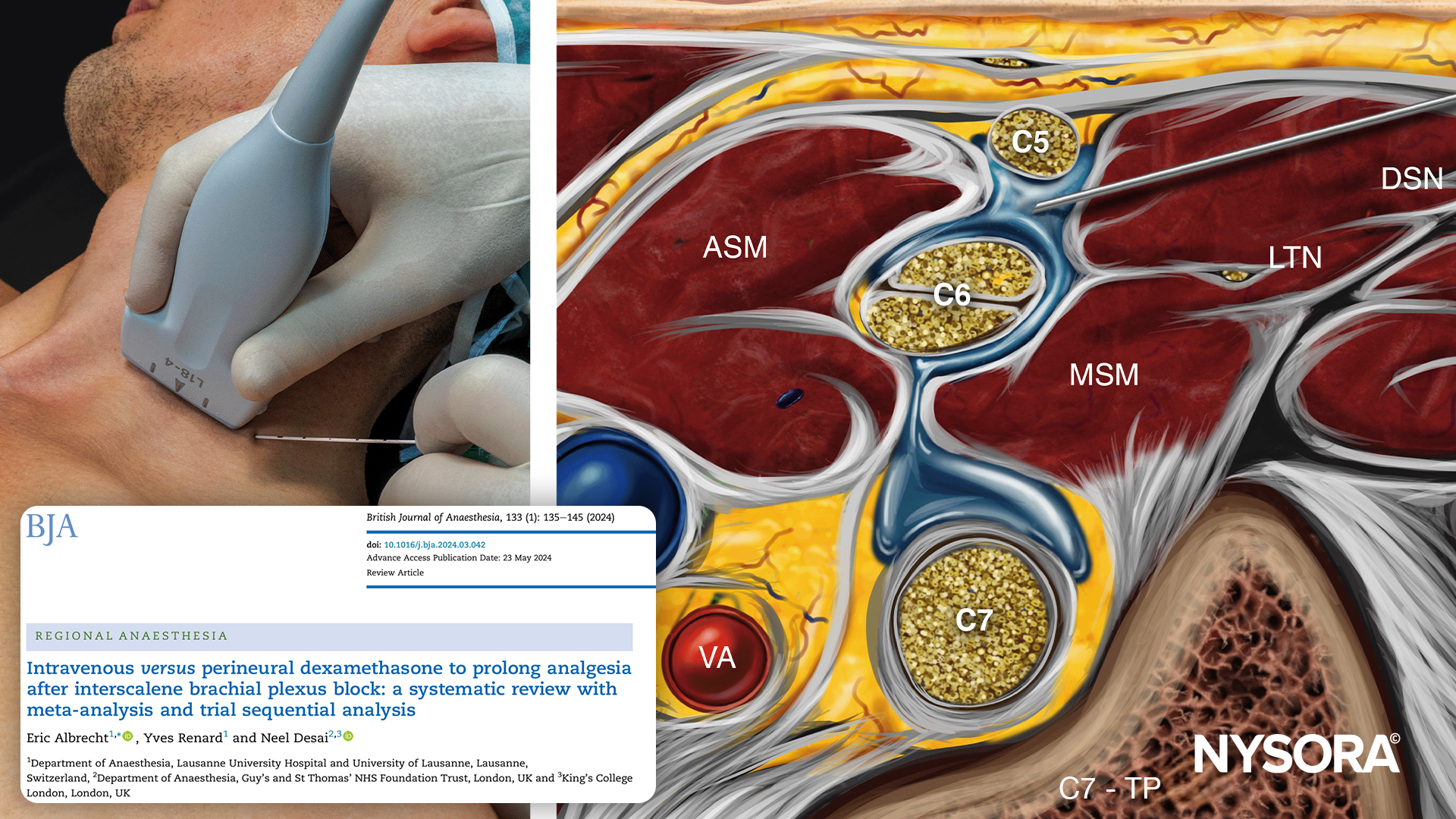
Introduction The interscalene brachial plexus block is a cornerstone for managing postoperative pain, particularly after shoulder surgeries. Enhancing the duration of analgesia is critical to patient comfort and recovery, and dexamethasone, a potent steroid, has been shown to play a significant role in this enhancement. However, the optimal route of administration—intravenous (IV) versus perineural—remains a topic of debate. This news post delves into a comprehensive systematic review and meta-analysis that compares these two administration routes, aiming to provide clarity for clinicians. Study overview Objective: To compare the efficacy of IV and perineural dexamethasone in prolonging analgesia after interscalene brachial plexus block. Design: A systematic review, meta-analysis, and trial sequential analysis. Participants: 11 trials involving 1145 patients undergoing shoulder surgery. Primary outcome: Duration of analgesia. Secondary outcomes: Onset time of sensory and motor blockade, pain scores at various time intervals, cumulative opioid consumption, and incidence of adverse effects. Key Findings Perineural dexamethasone significantly increased the duration of analgesia by an average of 2 hours compared to IV dexamethasone. Perineural administration also decreased the onset time for both sensory and motor blockade. Perineural dexamethasone resulted in lower pain scores at 12 hours post-surgery. No significant differences were observed in cumulative opioid consumption between the two groups. There were no significant differences in adverse effects, including nausea, vomiting, hyperglycemia, infection, and neurological complications. Discussion The findings suggest that while perineural dexamethasone offers a modest increase in analgesia duration, the clinical significance of this difference is debatable. Given the off-label status of perineural administration and the risk of crystallization when mixed with certain local anesthetics like ropivacaine, intravenous administration may be the safer and more practical option for most clinical settings. Conclusion This comprehensive review highlights the nuanced benefits and risks associated with the administration routes of dexamethasone in prolonging analgesia after interscalene brachial […]

Introduction Aortic valve disease, affecting around 3-4% of the Western population and up to 6% of those over 75, is a significant health concern. The only curative treatment is aortic valve replacement (AVR), which has evolved from open-heart surgery to minimally invasive techniques such as total endoscopic aortic valve replacement (TEAVR). Despite surgical advancements, postoperative pain management remains reliant on opioids, which have several side effects. This study explores the efficacy of the serratus anterior plane block (SAPB) in reducing opioid consumption and pain after TEAVR. Study overview Objective: To assess if SAPB can reduce opioid use and pain compared to standard care in TEAVR patients. Design: A prospective, double-blind, randomized controlled trial. Participants: 75 patients undergoing TEAVR, divided into SAPB and control groups. Primary outcome: Opioid consumption within the first 24 hours post-surgery. Secondary outcomes: Pain scores at 4, 8, and 24 hours post-surgery. Methodology Adult patients scheduled for TEAVR, excluding those with chronic pain, opioid dependence, or significant chest trauma. Patients were randomly assigned to receive SAPB plus standard care or standard care alone. Both patients and healthcare providers were blinded to group assignments. The SAPB group received a single injection of bupivacaine under ultrasound guidance targeting the serratus anterior plane. Results Median opioid use was significantly lower in the SAPB group (9 morphine milligram equivalents [MME]) compared to the control group (15 MME). The SAPB group reported lower pain scores at 4, 8, and 24 hours post-surgery. There were no significant differences in postoperative complications or length of hospital stay between groups. Discussion The study confirms that SAPB can significantly reduce opioid consumption and pain intensity after TEAVR. These findings align with previous research on SAPB’s efficacy in thoracic and cardiac surgery. However, further research is needed to optimize the timing, drugs, and dosage of SAPB and […]
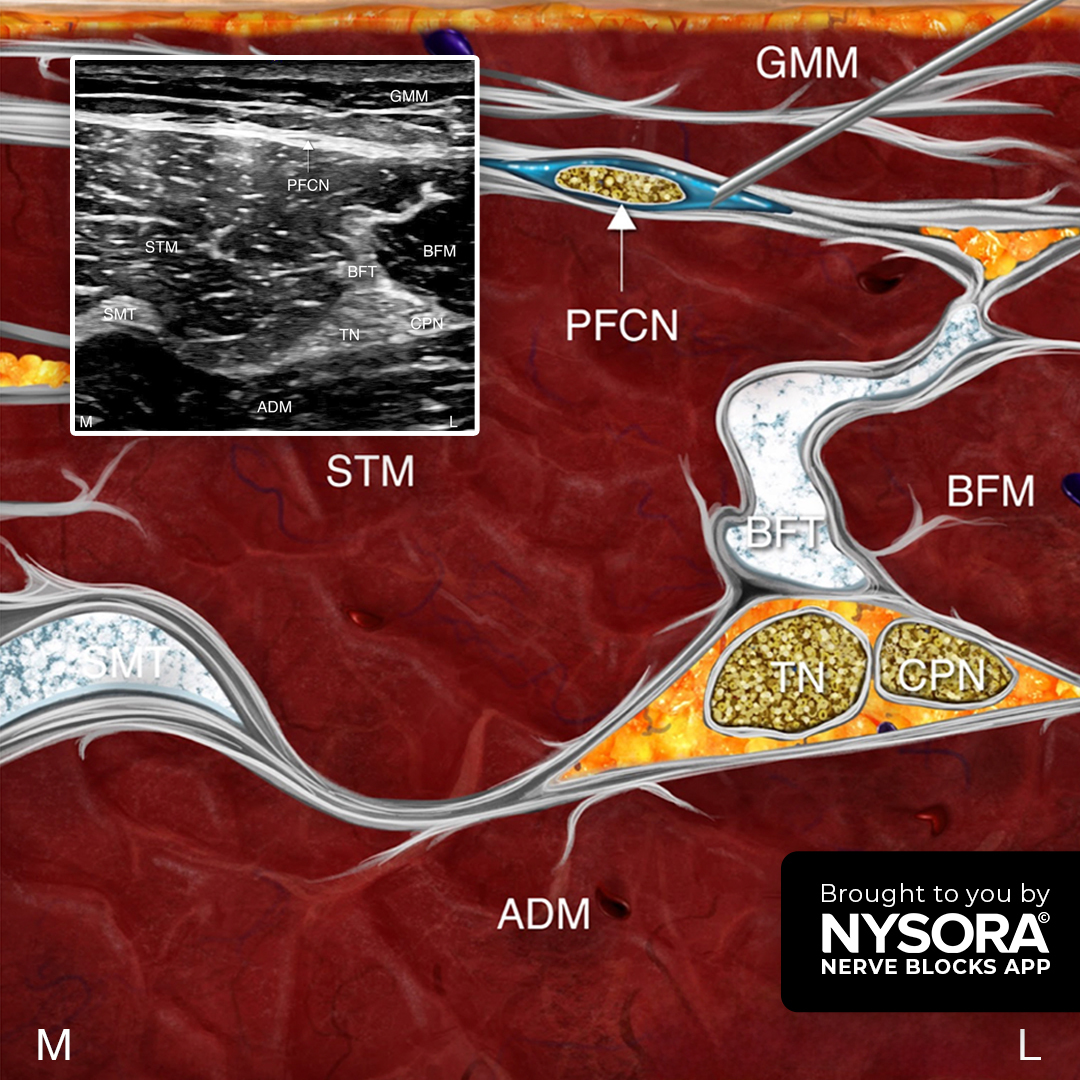
We added the Posterior Femoral Cutaneous Nerve (PFCN) Block technique to the NYSORA Nerve Blocks App. This advanced technique enhances pain management for surgeries involving the posterior thigh, knee, and lower leg. Technique overview The PFCN block is performed at the subgluteal crease or the popliteal fossa. It’s ideal for providing supplementary analgesia for procedures such as amputations above or below the knee, vein stripping, skin grafts, and ankle surgeries, especially when combined with sciatic and femoral/saphenous nerve blocks. Key points Goal: Local anesthetic spread around the nerve deep to the fascia lata Transducer: Linear Needle: 25-gauge, 2.5-4 cm Local anesthetic volume: 3-5 mL Patient position Subgluteal approach: Lateral decubitus or prone position Popliteal approach: Lateral decubitus, prone, or supine position with the calf elevated to maximize exposure of the popliteal fossa Learn how the Posterior Femoral Cutaneous Nerve Block can improve patient outcomes. Download the NYSORA Nerve Blocks App HERE for detailed guides, high-resolution images, and expert tips on this and numerous other nerve block techniques.
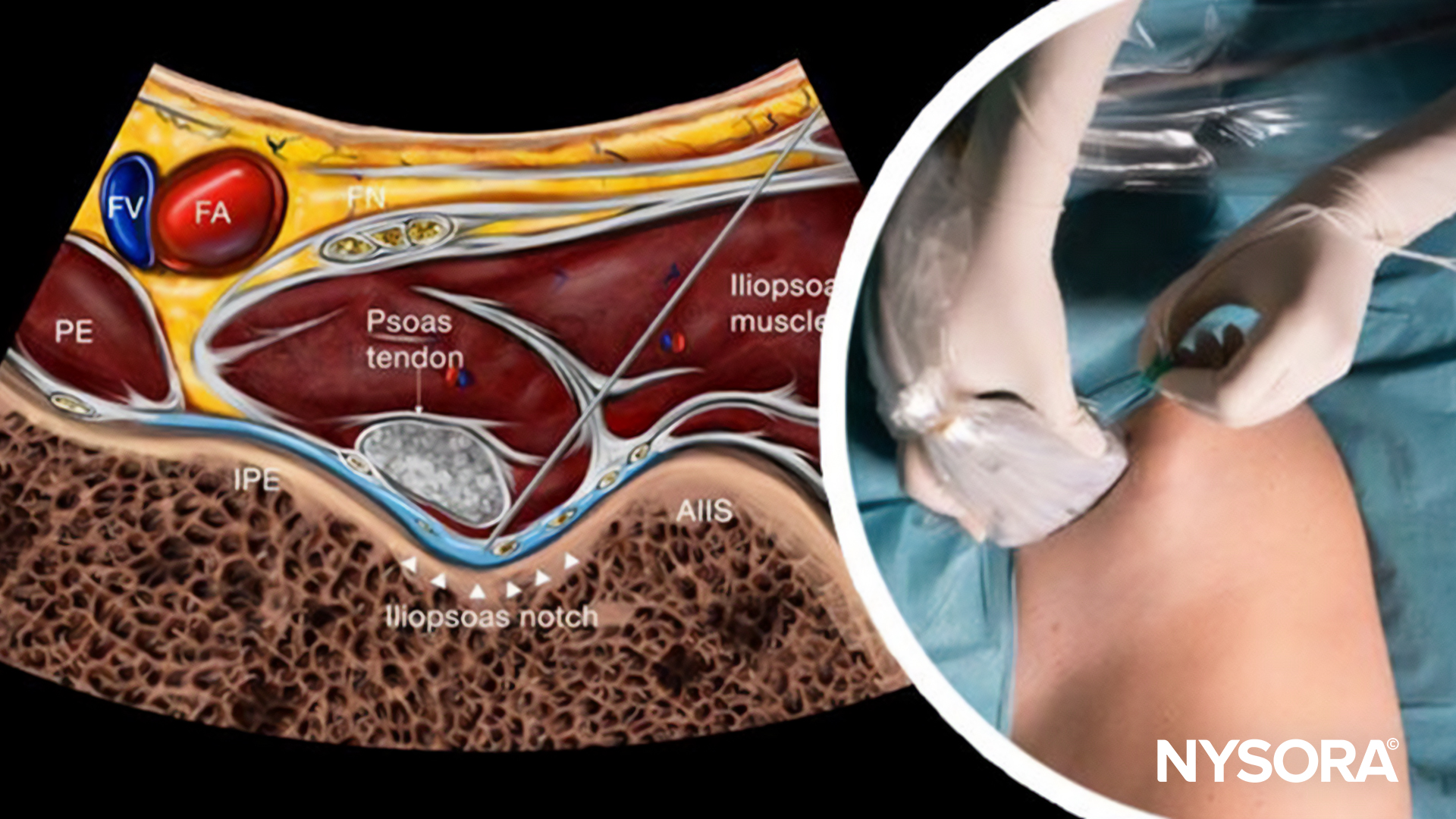
Introduction The pericapsular nerve group (PENG) block has emerged as a significant advancement in regional anesthesia, particularly for patients undergoing hip surgery. This motor-sparing analgesia technique was initially conducted in cadaver studies, which suggested its effectiveness in targeting specific nerve branches associated with the hip joint. The current study by Balocco et al. leverages 3D CT scan imaging to evaluate the distribution of local anesthetic in living patients, providing critical insights into the mechanism and efficacy of the PENG block. Rationale The PENG block is believed to target the articular branches of the femoral and accessory obturator nerves, providing analgesia to the hip joint. Prior investigations primarily utilized cadaver models, revealing that local anesthetics could reach the desired nerve branches. However, reports of quadriceps muscle weakness in clinical settings prompted further exploration into the actual spread of the injectate in live patients. Materials & Methods Ten patients scheduled for hip surgery were enrolled. Inclusion criteria included patients over 18, with an ASA physical status of I to III, and without severe systemic diseases. Patients received an ultrasound-guided PENG block using 20 mL of a mixture of 0.5% ropivacaine and radiopaque contrast. Following the block, a high-resolution CT scan provided a three-dimensional reconstruction of the injectate distribution. The block was administered with the patient in a supine position. Using ultrasound guidance, the needle was inserted to the plane just lateral to the psoas tendon. Following bone contact, the needle was slightly rotated to optimize injectate spread and avoid intramuscular injection. Results The injectate was mainly confined to the epimysium of the iliacus and the psoas muscle, with a minor spread to the hip capsule. Contrast dye was detected within the iliacus and/or the psoas muscle in all patients. No spread was observed to either the subpectineal plane or the obturator foramen. […]
Total knee arthroplasty (TKA) is a common surgical procedure for patients with severe knee osteoarthritis, aimed at alleviating pain and improving function. Effective postoperative pain management is critical for patient recovery, mobility, and satisfaction. Traditional multimodal analgesia for TKA often includes periarticular injections (PAI) of local anesthetics. However, a recent study by YaDeau et al., published in the Anesthesia & Analgesia journal, explores whether PAI is necessary when combined with adductor canal block (ACB) and infiltration between the popliteal artery and capsule of the knee (IPACK) blocks, questioning the necessity and efficacy of these injections. Study objective and methods The study objective was to evaluate the efficacy of PAI in reducing postoperative pain in patients undergoing TKA who were already receiving a multimodal analgesia regimen that included ACB and IPACK blocks. This randomized, blinded, placebo-controlled noninferiority trial enrolled 94 patients undergoing primary unilateral TKA. Participants were randomly assigned to receive either an active PAI (a mixture of bupivacaine, morphine, methylprednisolone, cefazolin, and saline) or a saline PAI (sham). All patients received a standardized multimodal analgesic protocol that included spinal anesthesia, ACB and IPACK blocks, intraoperative ketamine and ketorolac, and postoperative medications such as meloxicam, acetaminophen, duloxetine, and oral opioids. The primary outcome was pain with ambulation on postoperative day 1 (POD1), while secondary outcomes included opioid consumption, pain at rest, worst pain, pain interference, quality of recovery, patient satisfaction, length of hospital stay, chronic pain, and orthopedic outcomes. Key findings Primary outcome: Pain with ambulation on POD1 was not significantly different between patients receiving active PAI (with local anesthetic) and those receiving a saline PAI (sham) (4.26 ± 3.03 vs 4.55 ± 2.7, p=0.120). Secondary outcomes: No significant differences were observed in opioid consumption, pain at rest, worst pain, pain interference, quality of recovery, satisfaction, length of stay, chronic pain, […]
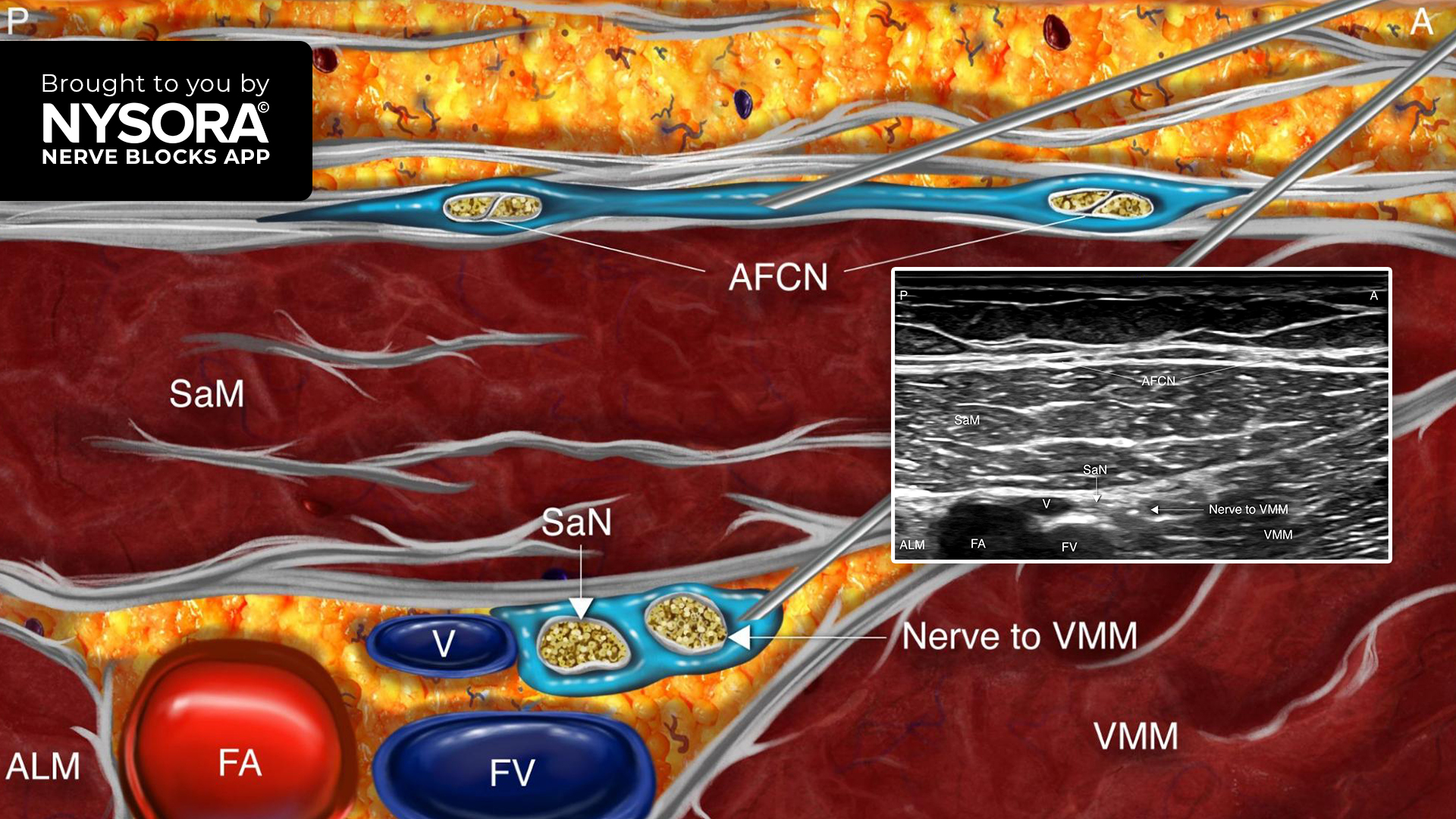
We added the Anterior Femoral Cutaneous Nerve (AFCN) Block technique to the NYSORA Nerve Blocks App. This innovative technique enhances pain management for anteromedial thigh and knee procedures. Technique overview The AFCN Block is performed at the anterior midthigh and is indicated for providing analgesia for surgeries on the anteromedial thigh and knee, such as skin grafting (in combination with the lateral femoral cutaneous nerve block) and supplementary analgesia for total knee arthroplasty (in combination with subsartorial blocks). Key points Goal: Achieve local anesthetic spread around the AFCN, superficial to the sartorius muscle, to ensure effective analgesia. Transducer: Linear Needle: 25-gauge, 2.5-4 cm Local anesthetic volume: 3-5 mL Patient position: Supine with the lower extremity extended for optimal exposure. Ready to enhance your practice with the latest in pain management techniques? Read more about the Anterior Femoral Cutaneous Nerve Block and how it can benefit your patients. Download the NYSORA Nerve Blocks App HERE to access detailed guides, high-resolution images, and expert tips for this and many other nerve block techniques.

Case description A 70-year-old female patient received a diagnosis of severe stenosis of the right internal carotid artery, necessitating a carotid endarterectomy to remove the atherosclerotic plaque. Due to her age and history of stroke, the surgical team opted for regional anesthesia to facilitate neurological monitoring throughout the procedure. Nerve block technique The patient was positioned supine with the neck slightly extended and rotated away from the side to be blocked. Using a high-frequency linear ultrasound transducer, the cervical plexus was visualized along the posterior border of the sternocleidomastoid muscle. Under ultrasound guidance, a 22-gauge, 50 mm needle was inserted in-plane. After negative aspiration and confirming correct needle placement, 10 mL of 0.25% bupivacaine was injected incrementally around the cervical plexus, while monitoring for signs of intravascular or intrathecal injection. Patient outcome The carotid endarterectomy was completed under the cervical plexus block, with the patient remaining alert and responsive throughout the surgery. Neurological monitoring during carotid artery clamping revealed no changes, underscoring the advantage of regional anesthesia. Postoperative pain was effectively controlled, and the procedure was free from complications. Exploring the Use of Intermediate Cervical Plexus Block in Carotid Endarterectomy: A Case Series Introduction Stroke is a leading cause of mortality worldwide, with carotid artery disease contributing to 10-20% of cases. Carotid endarterectomy is the recommended treatment for symptomatic patients with significant carotid stenosis to prevent embolic strokes. Traditionally, this procedure is carried out under general anesthesia or deep cervical plexus block (DCPB), both of which have their own set of complications. However, a recent case series by Ratnayake et al. 2024 highlights the potential of intermediate cervical plexus block (ICPB) combined with superficial cervical plexus block (SCPB) as a safer and more effective alternative. Materials and Methods This case series involved five patients with symptomatic carotid stenosis who underwent […]
Regional anesthesia numbs a specific area of the body, blocking pain in that region during and after surgical procedures. Unlike general anesthesia, which renders the patient unconscious, regional anesthesia allows the patient to remain awake or lightly sedated without feeling pain in the targeted area. This is achieved by inhibiting the transmission of pain signals to the brain.
Regional anesthesia has several benefits, such as minimized systemic opioid requirements, reduced postoperative pain and nausea, and improved recovery rates. It also decreases the risk of complications associated with general anesthesia, making it a preferred choice for specific patient populations and surgical interventions. Additionally, it can provide pain relief for several hours or days after the procedure.
Ultrasound-guided nerve blocks are a medical procedure used to alleviate pain by targeting specific nerves by administering local anesthetics or other therapeutic agents. Ultrasound imaging visualizes the nerves and surrounding structures in real-time, allowing for precise needle placement and injection.
Ultrasound-guided nerve blocks provide numerous advantages. They intensify accuracy and precision by enabling clear visualization of the targeted nerve and surrounding structures, minimizing the likelihood of errors in needle placement. This increases the efficacy of the procedure but also reduces the risk of complications such as inadvertent vascular puncture or nerve damage. Furthermore, the real-time visualization with ultrasound allows for immediate adjustments during needle placement, optimizing the delivery of medication and ensuring its effective localization.
Nerve blocks offer precise pain control in specific regions of the body for surgical procedures, trauma management, and pain interventions. By delivering anesthesia directly to the site of action, nerve blocks minimize systemic side effects associated with general anesthesia, improving patient safety and comfort. They can also reduce the need for general anesthesia, leading to shorter hospital stays, decreased opioid consumption, earlier mobilization, and faster recovery times. Moreover, these nerve blocks enhance surgical conditions by providing optimal anesthesia to the surgical site, thereby improving surgical outcomes and patient satisfaction.
The NYSORA Nerve Blocks App is designed to cater to a diverse global audience, ensuring that healthcare professionals worldwide can access its comprehensive educational content on nerve block techniques. As of the latest update, the app is available in multiple languages, including English, Spanish, Portuguese, Chinese, Japanese, French, Dutch, and German. This multilingual support underscores NYSORA's commitment to promoting excellence in regional anesthesia and pain management across different linguistic and cultural backgrounds.
Download the NYSORA Nerve Blocks app today and test drive the free blocks!




Join our mailing list and get weekly educational updates delivered straight to your inbox.