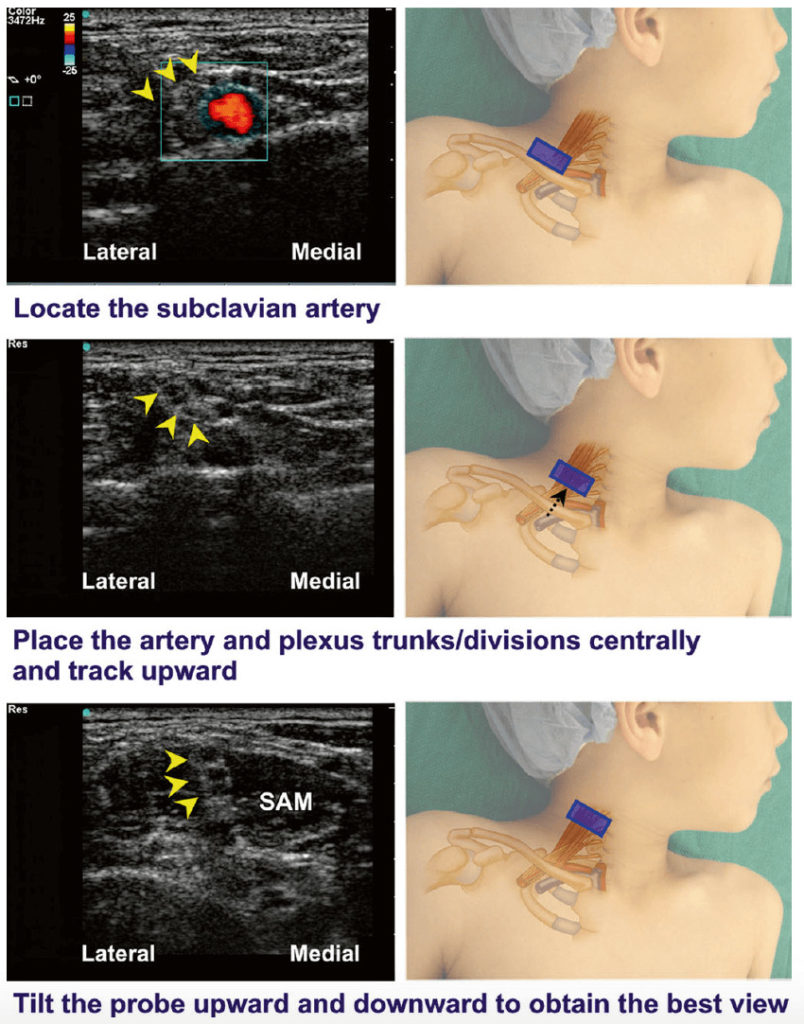
The probe is positioned in a coronal oblique plane at the midpoint to medial aspect of the upper border of the clavicle.
The pulsating subclavian artery becomes visible. (The probe may have to be moved laterally while maintaining contact with the clavicle). Doppler ultrasound can greatly assist with identification of this structure.
The probe is adjusted to place the subclavian artery in the center of the image. The brachial plexus (trunks/divisions) can be seen in short axis as a tightly enclosed cluster (i.e., a honeycomb-like arrangement), superior and lateral to the subclavian artery.
The image can be optimized by tilting the probe anteriorly or posteriorly.
The scanning angle is maintained as the plexus is traced in a cephalad direction along the interscalene groove to the level of the cricoid cartilage (C6) to reveal a transverse view of the neural structures located deep to the sternocleidomastoid muscle between the anterior and middle scalene muscles (Fig. 7).
Fig. 7 Ultrasound traceback approach for interscalene block.
Pediatric Atlas of Ultrasound and Nerve Stimulation-Guided Regional Anesthesia
Enriched with NextLevel CME™ technology: – Make notes in seconds and never lose them – Insert your own images, infographics – Add and watch videos inside your notes – Attach PDFs, articles, website links – Listen to the audio