Nerve Block Tip of the Week: Quadratus Lumborum (QL) 2 Block
November 1, 2022
This week, we’re discussing the role of quadratus lumborum (QL) 2 and sharing a 3-step guide to performing this block.
For the postoperative analgesia of patients who have undergone abdominal surgery, the QL 2 or posterior QL block provides analgesia for the ipsilateral anterior abdominal wall (T8-T12).
Here are 3 tips that will help you to successfully perform a QL 2 block
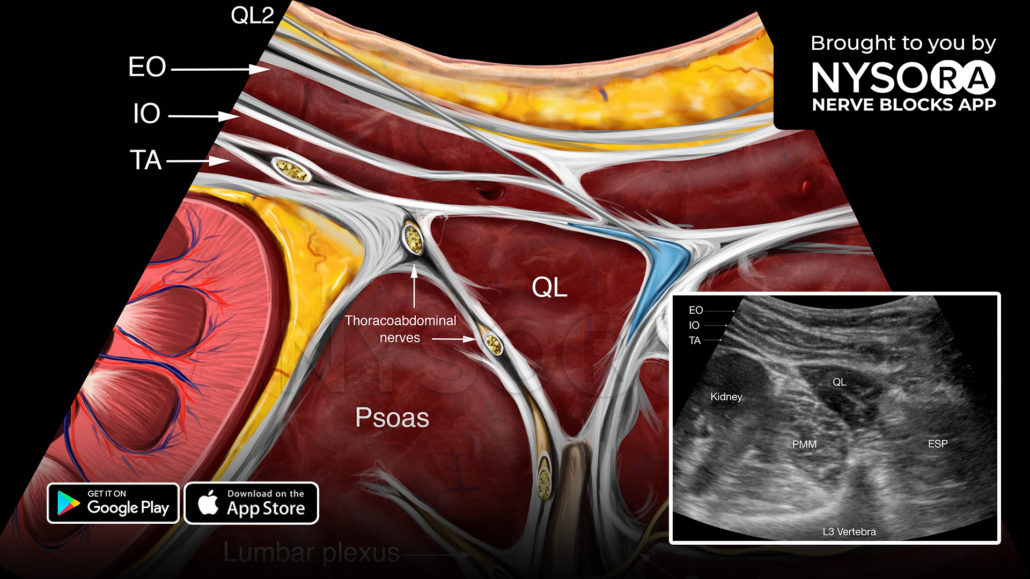
- Place the transducer in a transverse orientation at the midaxillary line and slide it posteriorly (similar to QL 1 block).
- Identify the fascial plane between the posterior aspect of the QL muscle and the middle layer of the thoracolumbar fascia.
- Insert the needle in-plane, from anterior to posterior, and inject 15-20 mL (0.2-0.3 mL/kg) of local anesthetic toward the posterior surface of the QL muscle.
Watch the video below to better understand the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE.