Case presentation A 44-year-old male patient presented with a history of a sports-related Achilles tendon tear. The tear was causing substantial pain, restricted mobility, and hindered his daily activities. The decision was made to proceed with Achil...
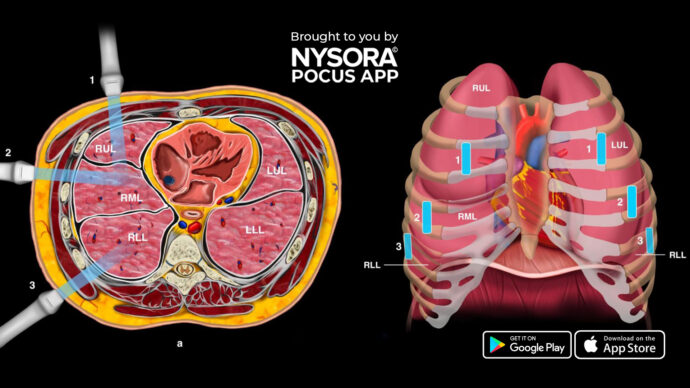
Lung consolidation refers to a condition where the air-filled spaces in the lung’s alveoli are replaced by fluid, pus, blood, or other substances. This results in the affected lung tissue becoming more solid and less able to exchange oxygen, le...
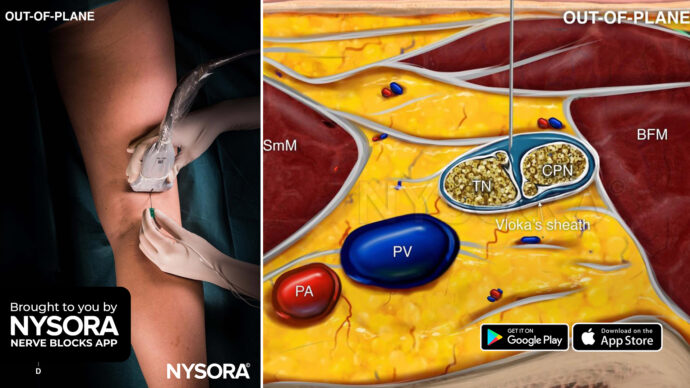
The popliteal sciatic nerve block is indicated for foot and ankle surgery, foot and toe amputation, and Achilles tendon surgery. It targets the sciatic nerve at or slightly above its division into the tibial and common peroneal nerves. The block can ...
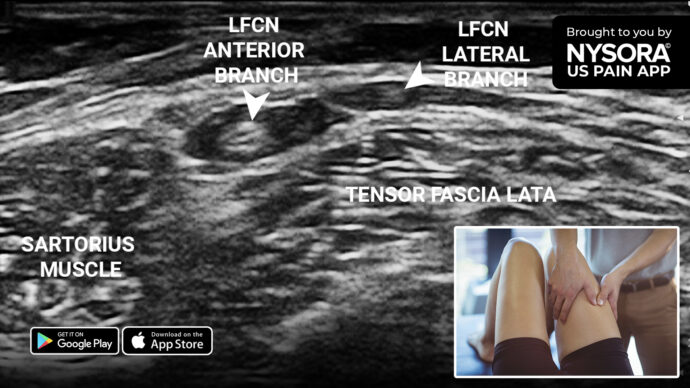
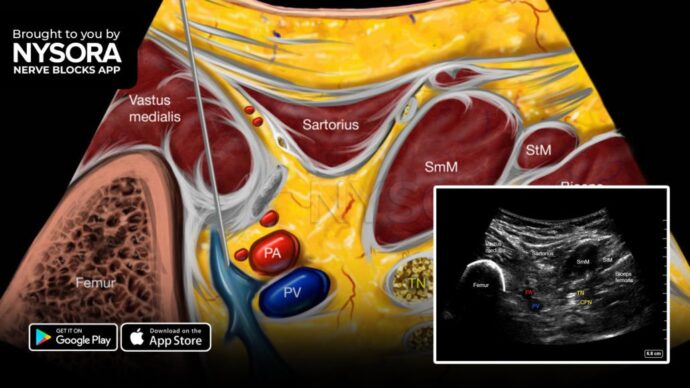
A 65-year-old woman, a homemaker, has been experiencing persistent pain and numbness in her right thigh for the past 5 years. A recent L4-L5 disc surgery provided no relief, and notably, the patient doesn’t recall any prior trauma. Physical exa...
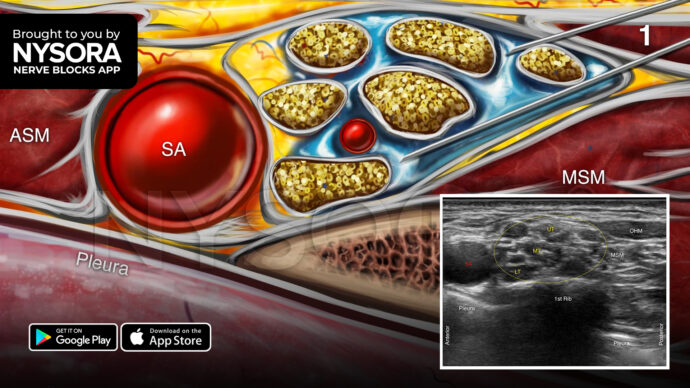
Case presentation A 52-year-old obese woman with chronic obstructive pulmonary disease (COPD) Gold III and a history of acute myocardial infarction (AMI) was scheduled for elbow surgery. The patient required an appropriate anesthetic approach that ta...
Here’s an intriguing paradox in regional anesthesia: While one might intuitively believe that slim patients would be easier subjects for an axillary brachial plexus block, the opposite seems to hold true. Why is this procedure more challenging in tho...
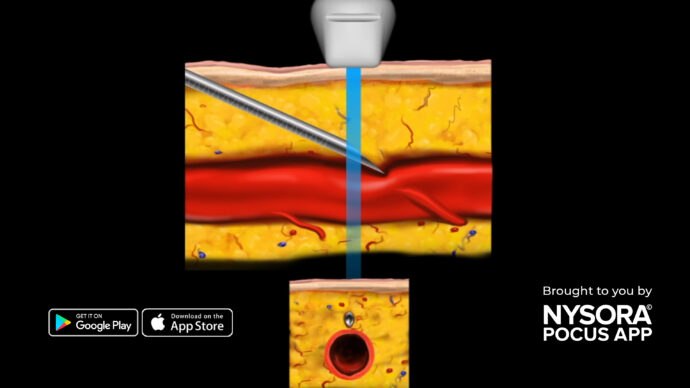
When conducting peripheral vascular access procedures, such as radial artery cannulation, executing the technique smoothly is crucial to reduce risks and enhance patient comfort. Proper visualization of the needle tip is essential when performing an ...
IPACK stands for Infiltration of local anesthetic between the Popliteal Artery and Capsule of the Knee. It is a motor-sparing technique that anesthetizes the small articular sensory nerves from the popliteal plexus and obturator nerve resulting in an...
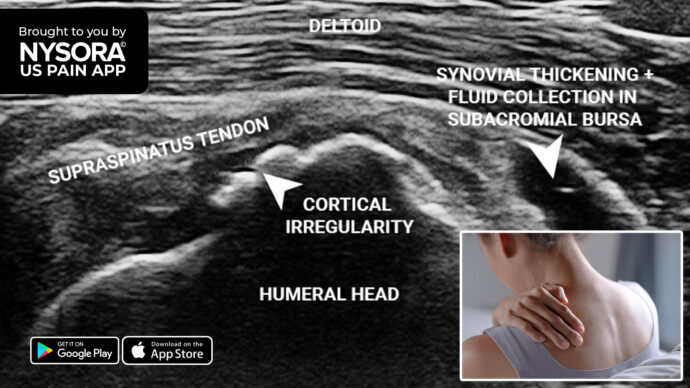
A 46-year-old woman presented with chronic shoulder pain persisting for 8 months after a minor injury. Night pain and incidental pain during internal rotation and shoulder abduction were her main complaints. The pain primarily centered around the sup...
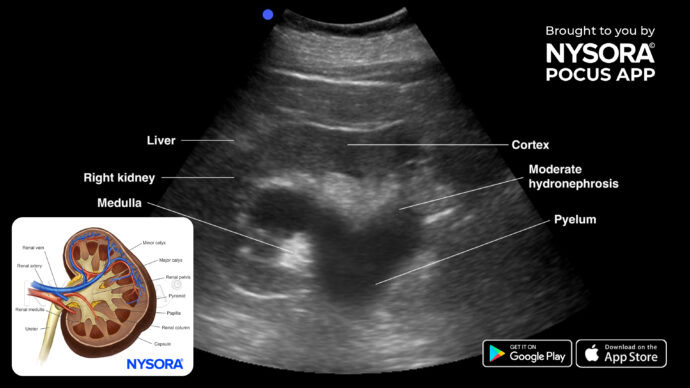
Hydronephrosis is characterized by obstructive uropathy and thus enlargement of one or both kidneys due to the build-up of urine. Potential causes include kidney or bladder stones, benign prostatic hyperplasia (BPH), various cancers (bladder, renal, ...