Patient Case Study: De Quervain’s Tenosynovitis – Injection
Case presentation
A 56-year-old lady presents with a history of chronic pain in her left hand for six months. She has worked in a printing press for the last 6 years. No history of hand injury.
Diagnosis
Physical exam
Finkelstein’s test was positive. In the Finkelstein test, the patient is asked to bend the thumb across the palm of the hand and bend the fingers down over the thumb. The patient is then asked to bend the wrist toward the little finger (ulnar deviation of the wrist). If this causes pain on the thumb side of the wrist, the patient likely has de Quervain tenosynovitis.
Ultrasound findings
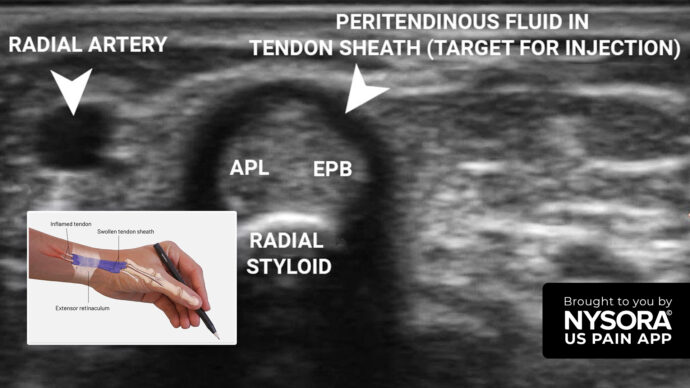
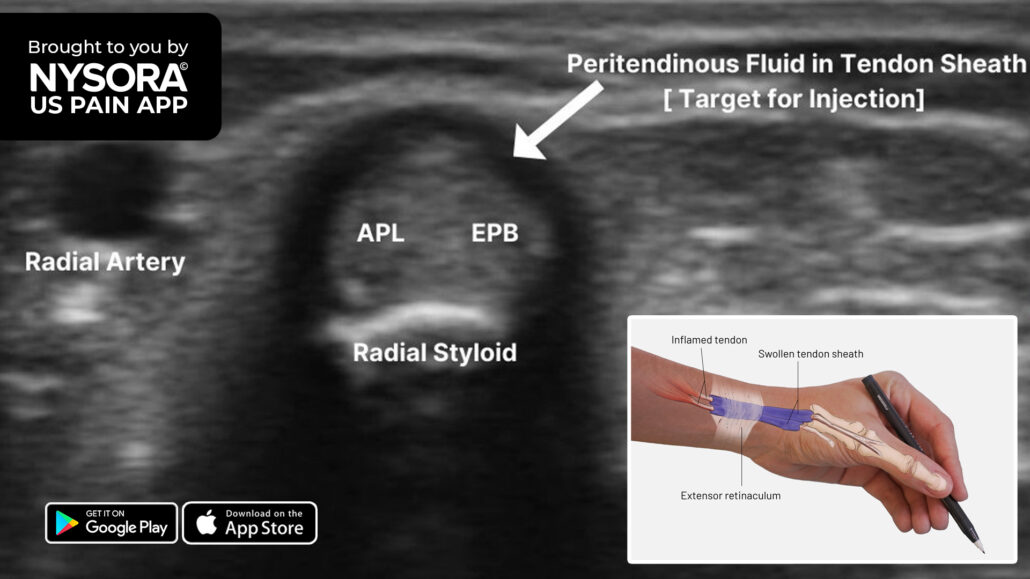
Transverse view of extensor compartment 1 showing a surrounding thin rim of inflammatory fluid. APL, abductor pollicis longus; EPB, extensor pollicis brevis.

Longitudinal view of extensor compartment 1 showing swollen tendons and a surrounding thin rim of inflammatory fluid. APL, abductor pollicis longus; EPB, extensor pollicis brevis.
Diagnosis
De Quervain’s tenosynovitis.
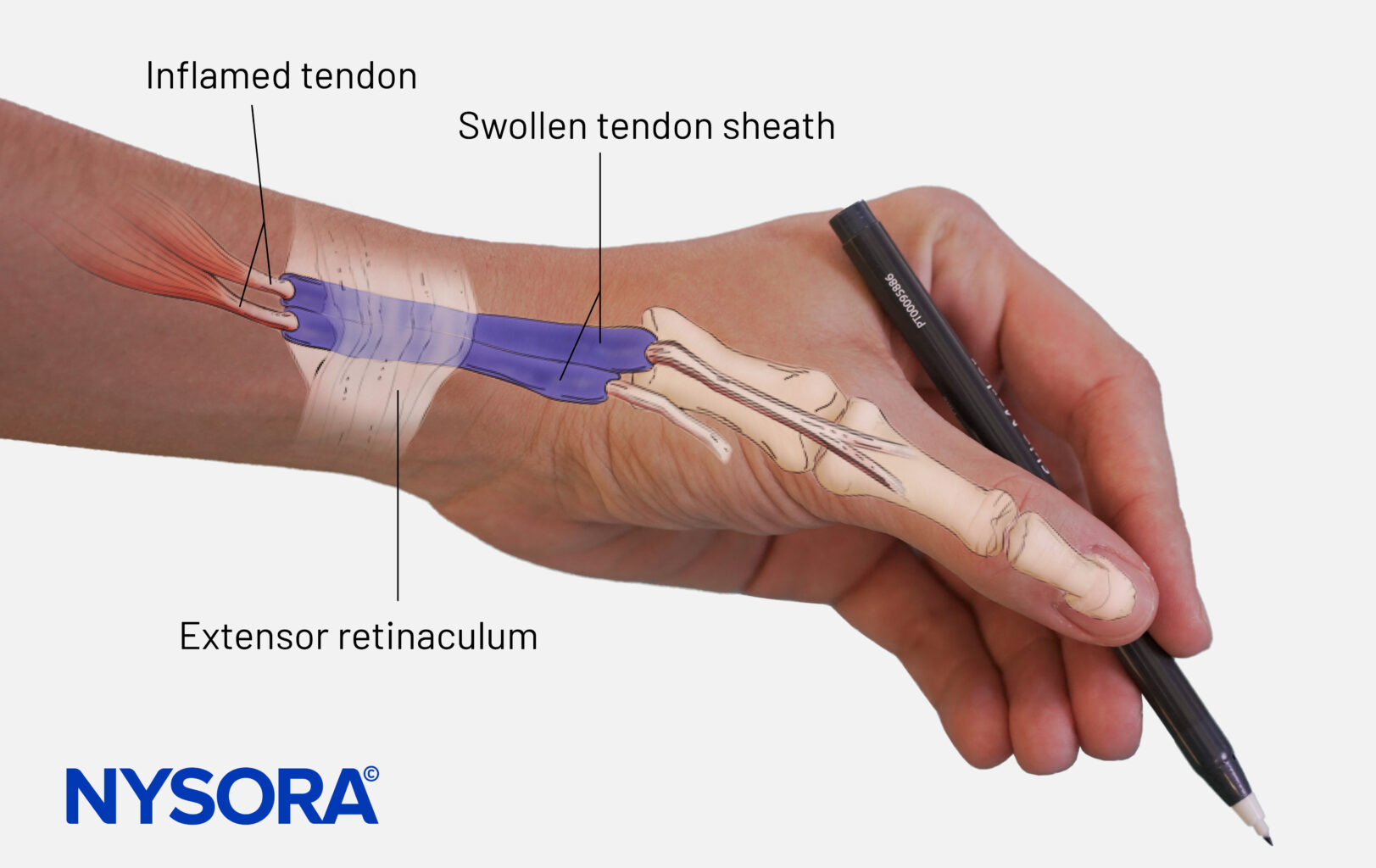
Definition: De Quervain’s tenosynovitis is characterized by swelling of the tendons that run along the thumb side of the wrist and attach to the base of the thumb (abductor pollicis longus and extensor pollicis brevis). This occurs when the tendons are constricted by the sheath they run through from the wrist to the hand.
Treatment
Technique description
Extensor compartment 1 tendon sheath injection over the wrist:
In axial imaging of the extensor compartment 1 tendons, a 24 gauge 1.25-inch needle is inserted with aseptic precautions after infiltration anesthesia with 1% lidocaine. After entering the extensor tendon sheath, 1 mL of 1% lidocaine is injected along with 10 mg of triamcinolone. Care should be taken to avoid injecting steroids into the tendon per se.
Indications
For pain relief.
Anatomy
Transverse view of extensor compartment 1 showing a surrounding thin rim of inflammatory fluid. APL, Abductor pollicis longus; EPB, extensor pollicis brevis.
Technique
Ultrasound machine setup
- <strong>Transducer type:</strong> 3 -13 MHz, linear transducer. Hockey stick probe is better for needling.
- <strong>Ultrasound preset:</strong> Musculoskeletal
- <strong>Orientation:</strong> Axial
- <strong>Depth:</strong> 1 cm
Patient position
Supine, wrist in the semi-pronated position. Place a gel tube under the wrist.
Landmarks
Transverse view of extensor compartment 1 showing a surrounding thin rim of inflammatory fluid. APL, Abductor pollicis longus; EPB, extensor pollicis brevis.
Transducer position
![]()
Scanning
With the wrist and forearm in the semi-pronated position, place a small gel tube underneath to achieve a minimal ulnar deviation of the wrist which will provide a better image avoiding anisotropy. Plenty of stand-off gel without much transducer pressure will help make the diagnosis easier. The linear transducer is placed over the radial styloid in the axial plane. Inflammatory fluid can be seen around the tendons. Neoangiogenesis can be appreciated with color Doppler study. A long-axis dynamic study of the tendons will help evaluate the echotexture and integrity of the tendon.
Transverse view of extensor compartment 1 showing a surrounding thin rim of inflammatory fluid. APL, Abductor pollicis longus; EPB, extensor pollicis brevis.
Longitudinal view of extensor compartment 1 showing swollen tendons and a surrounding thin rim of inflammatory fluid. APL, abductor pollicis longus; EPB, extensor pollicis brevis.
Color Doppler examination of extensor compartment 1 showing increased vascularity due to inflammation.
Needle insertion
After sterile preparations of the wrist, hand, and transducer, a 24 gauge 1.25-inch hypodermic needle is inserted after local anesthetic infiltration. Only 0.5 mL of 2% lidocaine is used for infiltration to avoid distorting the plane of injection. A lateral to medial needling is performed to enter the extensor compartment. Care is taken to avoid the radial artery and the tendons within. 1 mL of 1 percent lidocaine with 10 mg triamcinolone is injected within the sheath. A needle fenestration may be attempted to release the extensor retinaculum above the APL and EPB tendons.

Extensor compartment 1 injection. APL, abductor pollicis longus; EPB, extensor pollicis brevis; RA, radial artery.
Pharmacological agents
1 mL of 1% lidocaine with 10 mg triamcinolone.
Patient outcome
100% pain relief 1 week after the intervention with complete functional restoration. No procedural complications.
Contributor
Dr. Madhan Pandian., MD., CIPS., RMSK
Senior Specialist, IGGGH & PGI and National Board of Examinations,
MSK Interventional Pain Sonologist,
Pain Speciality Clinic