


Benaifer D. Preziosi, Adam T. Hershkin, Paul J. Seider, and Gregory M. Casey
INTRODUCTION
Oral surgical and dental procedures are often performed in an outpatient setting. Regional anesthesia is the most common method of anesthetizing the patient before office-based procedures.
Several highly efficacious and practical techniques can be used to achieve anesthesia of the dentition and surrounding the hard and soft tissues of the maxilla and mandible. The type of procedure to be performed as well as the location of the procedure determine the technique of anesthesia to be used. Orofacial anesthetic techniques can be classified into three main categories: local infiltration, a field block, and nerve block.
The local infiltration technique anesthetizes the terminal nerve endings of the dental plexus (Figure 1).

Figure 1. Anatomy of the trigeminal nerve. The sensory root of the trigeminal nerve gives rise to the ophthalmic division (V1), maxillary division (V2), and mandibular division (V3) from the trigeminal ganglion.
This technique is indicated when an individual tooth or a specific isolated area requires anesthesia. The procedure is performed within the direct vicinity of the site of infiltration.
The field block anesthetizes the terminal nerve branches in the area of treatment. Treatment can then be performed in an area slightly distal to the site of injection. Dental and maxillofacial practitioners often use the deposition of local anesthetic at the apex of a tooth for the purposes of achieving pulpal and soft tissue anesthesia. Although this is commonly termed “local infiltration,” since the terminal. Terminal nerve branches are anesthetized in this technique, such infiltration is more correctly termed as field block. In contrast, the nerve block anesthetizes the main branch of a specific nerve, allowing treatment to be performed in the region innervated by the nerve.
This section reviews the essential anatomy of orofacial nerves and details the practical approaches to performing nerve blocks and infiltration anesthesia for a variety of surgical procedures in this region.
ANATOMY OF THE TRIGEMINAL NERVE
General Considerations
Anesthesia of the teeth and the soft and hard tissues of the oral cavity can be achieved with block of the branches of the trigeminal nerve (fifth cranial nerve). In fact, regional, field, and local anesthesia of the maxilla and mandible is accomplished by the deposition of the anesthetic solution near terminal nerve branches or a main nerve trunk of the trigeminal nerve.
The largest of all the cranial nerves, the trigeminal nerve gives rise to a small motor root, originating in the motor nucleus within the pons and medulla oblongata, and a larger sensory root, which finds its origin in the anterior aspect of the pons (see Figure 1). The nerve travels forward from the posterior cranial fossa to the petrous portion of the temporal bone within the middle cranial fossa. Here, the sensory root forms the trigeminal (semilunar or gasserian) ganglion, situated within Meckel’s cavity on the anterior surface of the petrous portion of the temporal bone. The ganglia are paired, with one innervating each side of the face. The sensory root of the trigeminal nerve gives rise to the ophthalmic division (V1), the maxillary division (V2), and the mandibular division (V3) from the trigeminal ganglion (see Figure 1).
The motor root travels from the brainstem along with, but separate from, the sensory root. It then leaves the middle cranial fossa through the foramen ovale after passing underneath the trigeminal ganglion in a lateral and inferior direction. The motor root exits the middle cranial fossa along with the third division of the sensory root: the mandibular nerve. It then unites with the mandibular nerve to form a single nerve trunk after exiting the skull. The motor fibers supply the muscles of mastication (masseter, temporalis, medial pterygoid, and lateral pterygoid) and the mylohyoid, anterior belly of the digastric, tensor veli palatine, and tensor tympani muscles.
The Ophthalmic Division
The smallest of the three divisions, the ophthalmic division (V1) is purely sensory and travels anteriorly in the lateral wall of the cavernous sinus in the middle cranial fossa to the medial part of the superior orbital fissure. Before its entrance into the orbit through the superior orbital fissure, the ophthalmic nerve divides into three branches: the frontal, nasociliary, and lacrimal.
The frontal nerve is the largest branch of the ophthalmic division and travels anteriorly in the orbit, terminating as the supratrochlear and supraorbital nerves. The supratrochlear nerve lies medial to the supraorbital nerve and supplies the skin and conjunctiva of the medial portion of the upper eyelid and skin over the lower forehead close to the midline. The supraorbital nerve supplies the skin and conjunctiva of the central portion of the upper eyelid, the skin of the forehead, and the scalp as far back as the parietal bone and lambdoid suture.
The nasociliary branch travels along the medial aspect of the orbital roof, giving off various branches. The nasal cavity and the skin at the apex and ala of the nose are innervated by the anterior ethmoid and external nasal nerves. The internal nasal nerve innervates the mucous membrane of the anterior portion of the nasal septum and lateral wall of the nasal cavity. The infratrochlear branch innervates the skin of the lacrimal sac, lacrimal caruncle, and adjoining portion of the side of the nose. The posterior ethmoidal nerve supplies the ethmoid and sphenoid sinuses. The short and long ciliary nerves innervate the eyeball.
The lacrimal nerve supplies the skin and conjunctiva of the lateral portion of the upper eyelid and is the smallest branch of the ophthalmic division.
Learn more about Local and Regional Anesthesia for Ophthalmic Surgery.
The Maxillary Division
The maxillary division (V2) of the trigeminal nerve is also a purely sensory division. Arising from the trigeminal ganglion in the middle cranial fossa, the maxillary nerve travels forward along the lateral wall of the cavernous sinus. Shortly after stemming from the trigeminal ganglion, the maxillary nerve gives off the only branch within the cranium: the middle meningeal nerve. It then leaves the cranium through the foramen rotundum, located in the greater wing of the sphenoid bone. After exiting the foramen rotundum, the nerve enters a space located behind and below the orbital cavity known as the pterygopalatine fossa. After giving off several branches within the fossa, the nerve enters the orbit through the inferior orbital fissure, at which point it becomes the infraorbital nerve. Coursing along the floor of the orbit in the infraorbital groove, the nerve enters the infraorbital canal and emerges onto the face through the infraorbital foramen.
The middle meningeal nerve is the only branch of the maxillary division within the cranium; it provides sensory innervation to the dura mater in the middle cranial fossa. Within the pterygopalatine fossa, several branches are given off, including the pterygopalatine, zygomatic, and posterior superior alveolar nerves. The pterygopalatine nerves are two short nerves that merge within the pterygopalatine ganglion and then give rise to several branches. They contain postganglionic parasympathetic fibers, which pass along the zygomatic nerve to the lacrimal nerve innervating the lacrimal gland, as well as sensory fibers to the orbit, nose, palate, and pharynx. The sensory fibers to the orbit innervate the orbital periosteum.
The nasal branches innervate the posterior aspect of the nasal septum, mucous membrane of the superior and middle conchae, and the posterior ethmoid sinus. The anterior nasal septum, floor of the nose, and premaxilla from canine to canine are innervated by a branch known as the nasopalatine nerve. The nasopalatine nerve courses downward and forward from the roof of the nasal cavity to the floor to enter the incisive canal. It then enters the oral cavity through the incisive foramen to supply the palatal mucosa of the premaxilla.
The hard and soft palate are innervated by the palatine branches: the greater (anterior) and lesser (middle and posterior) palatine nerves. After descending through the pterygopalatine canal, the greater palatine nerve exits the greater palatine foramen onto the hard palate. The nerve provides sensory innervation to the palatal mucosa and bone of the hard and soft palate. The lesser palatine nerves emerge from the lesser palatine foramen to innervate the soft palate and tonsillar region.
The pharyngeal branch leaves the pterygopalatine ganglion from its posterior aspect to innervate the nasopharynx.
The zygomatic nerve gives rise to two branches after passing anteriorly from the pterygopalatine fossa to the orbit. The nerve passes through the inferior orbital fissure and divides into the zygomaticofacial and zygomaticotemporal nerves, supplying the skin over the malar prominence and skin over the side of the forehead, respectively. The zygomatic nerve also communicates with the ophthalmic division via the lacrimal nerve, sending fibers to the lacrimal gland.
The posterior superior alveolar (PSA) nerve branches off within the pterygopalatine fossa before the maxillary nerve enters the orbit. The PSA travels downward along the posterior aspect of the maxilla to supply the maxillary molar dentition, including the periodontal ligament and pulpal tissues, as well as the adjacent gingiva and alveolar process. The PSA also innervates the mucous membrane of the maxillary sinus. It is of clinical significance to note that the PSA does not always innervate the mesiobuccal root of the first molar. Several dissection studies have been performed tracing the innervation of the first molar back to the parent trunk. These studies have demonstrated the variations in innervation patterns of the first molar, and this is of clinical significance when anesthesia of this tooth is desired.
In a study by Loetscher and Walton, 29 human maxillae were dissected to observe innervation patterns of the first molar. The study evaluated the innervation patterns by the posterior, middle, and anterior superior alveolar nerves on the first molar.
The posterior and anterior superior alveolar nerves were found to be present in 100% (29/29) of specimens. The middle superior alveolar (MSA) nerve was found to be present 72% of the time (21/29 specimens). Nerves were traced from the first molar to the parent branches in 18 of the specimens. The PSA nerve was found to provide innervation in 72% (13/18) of specimens. The MSA nerve provided innervation in 28% (5/18) specimens, whereas the anterior superior alveolar nerve did not provide innervation to the first molar in any of the specimens. In the absence of the MSA nerve, the PSA nerve may provide innervation to the premolar region. In a study by McDaniel, 50 maxillae were decalcified and dissected to demonstrate the innervation patterns of maxillary teeth. The PSA nerve was found to innervate the premolar region in 26% of dissections when the MSA nerve was not present. Table 1 lists the branches of the ophthalmic, maxillary, and mandibular divisions.
TABLE 1. Branches of three major divisions.
| Ophthalmic Division | Maxillary Division | Mandibular Division |
|---|---|---|
| 1.Frontal • Supratrochlear • Supraorbital | 1.Middle meningeal | 1.Main trunk • Nervous spinosus • Nerve to the pterygoid |
| 2.Nasociliary • Anterior ethmoid • External nasal • Internal nasal • Infratrochlear • Posterior ethmoid • Short and long ciliary | 2.Pterygopalatine nerves • Sensory fibers to the orbit • Nasal branches • Nasopalatine nerve • Greater palatine nerve • Lesser palatine nerve • Pharyngeal branch | 2.Anterior division • Masseteric • Deep temporal • Lateral pterygoid • Buccal nerve |
| 3.Lacrimal | 3.Zygomatic • Zygomaticofacial • Zygomaticotemporal | 3.Posterior division • Auriculotemporal • Lingual • Inferior alveolar • Nerve to the mylohyoid |
| 4.Posterior superior alveolar nerve | ||
| 5.Infraorbital • Middle superior alveolar • Anterior superior alveolar • Inferior palpebral • Lateral nasal • Superior labial |
Within the infraorbital canal, the maxillary division is known as the infraorbital nerve and gives off the middle and anterior superior alveolar nerves. When present, the MSA nerve descends along the lateral wall of the maxillary sinus to innervate the first and second premolar teeth. It provides sensation to the periodontal ligament, pulpal tissues, gingiva and alveolar process of the premolar region, as well as the mesiobuccal root of the first molar in some cases. In a study by Heasman, dissections of 19 human cadaver heads were performed, and the MSA was found to be present in seven specimens. Loetscher and Walton3 found that the mesial or distal position at which the MSA nerve joins the dental plexus (an anastomosis of the posterior, middle, and anterior superior alveolar nerves described below) determines its contribution to the innervation of the first molar. Specimens in which the MSA joined the plexus mesial to the first molar were found to have innervation of the first molar by the PSA and the premolars by the MSA.
Specimens in which the MSA joined the plexus distal to the first molar demonstrated innervation of the first molar by the MSA. In its absence, the premolar region derives its innervation from the PSA and anterior superior alveolar nerves. The anterior superior alveolar nerve descends within the anterior wall of the maxillary sinus. A small terminal branch of the anterior superior alveolar nerve communicates with the MSA to supply a small area of the lateral wall and floor of the nose. It also provides sensory innervation to the periodontal ligament, pulpal tissue, gingiva, and the alveolar process of the central and lateral incisor and canine teeth. In the absence of the MSA, the anterior superior alveolar nerve has been shown to provide innervation to the premolar teeth. In the previously mentioned study by McDaniel, the anterior superior alveolar nerve was shown to provide innervation to the premolar region in 36% of specimens in which no MSA nerve was found.
The three superior alveolar nerves anastomose to form a network known as the dental plexus, which comprises terminal branches coming off the larger nerve trunks. These terminal branches are known as the dental, interdental, and interradicular nerves. The dental nerves innervate each root of each individual tooth in the maxilla by entering the root through the apical foramen and supplying sensation to the pulp. Interdental and interradicular branches provide sensation to the periodontal ligaments, interdental papillae, and buccal gingiva of adjacent teeth.
The infraorbital nerve divides into three terminal branches after emerging through the infraorbital foramen onto the face. The inferior palpebral, external nasal, and superior labial nerves supply sensory innervation to the skin of the lower eyelid, lateral aspect of the nose, and skin and mucous membranes of the upper lip, respectively.
The Mandibular Division
The largest branch of the trigeminal nerve, the mandibular branch (V3), is both sensory and motor (Figure 2). The sensory root arises from the trigeminal ganglion, whereas the motor root arises from the motor nucleus of the pons and medulla oblongata. The sensory root passes through the foramen ovale almost immediately after coming off the trigeminal ganglion. The motor root passes underneath the ganglion and through the foramen ovale to unite with the sensory root just outside the cranium, forming the main trunk of the mandibular nerve. The nerve then divides into anterior and posterior divisions. The mandibular nerve gives off branches from its main trunk as well as from the anterior and posterior divisions.

Figure 2. Anatomy of the mandibular nerve.
The main trunk gives off two branches known as the nervus spinosus (meningeal branch) and the nerve to the medial pterygoid. After branching off the main trunk, the nervus spinosus reenters the cranium, along with the middle meningeal artery, through the foramen spinosum. The nervus spinosus supplies the meninges of the middle cranial fossa as well as the mastoid air cells. The nerve to the medial pterygoid is a small motor branch that supplies the medial (internal) pterygoid muscle. It gives off two branches that supply the tensor tympani and tensor veli palatini muscles. Three motor branches and one sensory branch are given off by the anterior division of the mandibular nerve. The masseteric, deep temporal, and lateral pterygoid nerves supply the masseter, temporalis, and lateral (external) pterygoid muscles, respectively. The sensory division known as the buccal (buccinator or long buccal) nerve, runs forward between the two heads of the lateral pterygoid muscle, along with the inferior aspect of the temporalis muscle to the anterior border of the masseter muscle. Here, it passes anterolaterally to enter the buccinator muscle; however, it does not innervate this muscle. The buccinator muscle is innervated by the buccal branch of the facial nerve. The buccal nerve provides sensory innervation to the skin of the cheek, buccal mucosa, and buccal gingiva in the mandibular molar region. The posterior division of the mandibular branch gives off two sensory branches (the auriculotemporal and lingual nerves) and one branch made up of both sensory and motor fibers (the inferior alveolar nerve).
The auriculotemporal nerve crosses the superior portion of the parotid gland, ascending behind the temporomandibular joint and giving off several sensory branches to the skin of the auricle, external auditory meatus, tympanic membrane, temporal region, temporomandibular joint, and parotid gland via postganglionic parasympathetic secretomotor fibers from the otic ganglion.
The lingual nerve travels inferiorly in the pterygomandibular space between the medial aspect of the ramus of the mandible and the lateral aspect of the medial pterygoid muscle. It then travels anteromedially below the inferior border of the superior pharyngeal constrictor muscle deep to the pterygomandibular raphae. The lingual nerve then continues anteriorly in the submandibular region along the hyoglossus muscle, crossing the submandibular duct inferiorly and medially to terminate deep to the sublingual gland. The lingual nerve provides sensory innervation to the anterior two-thirds of the tongue, mucosa of the floor of the mouth, and lingual gingiva.
The inferior alveolar branch of the mandibular nerve descends in the region between the lateral aspect of the sphenomandibular ligament and the medial aspect of the ramus of the mandible. It travels along with, but lateral and posterior to, the lingual nerve. While the lingual nerve continues to descend within the pterygomandibular space, the inferior alveolar nerve enters the mandibular canal through the mandibular foramen. Just before entering the mandibular canal, the inferior alveolar nerve gives off a motor branch known as the mylohyoid nerve (discussed below). The nerve accompanies the inferior alveolar artery and vein within the mandibular canal and divides into the mental and incisive nerve branches at the mental foramen. The inferior alveolar nerve provides sensation to the mandibular posterior teeth.
The incisive nerve is a branch of the inferior alveolar nerve that continues within the mandibular canal to provide sensory innervation to the mandibular anterior teeth.
The mental nerve emerges from the mental foramen to provide sensory innervation to the mucosa in the premolar/canine region, as well as to the skin of the chin and lower lip.
The mylohyoid nerve branches off the inferior alveolar nerve before its entry into the mandibular canal. It travels within the mylohyoid groove and along the medial aspect of the body of the mandible to supply the mylohyoid muscle as well as the anterior belly of the digastric muscle.
EQUIPMENT FOR REGIONAL MAXILLARY & MANDIBULAR ANESTHESIA
Administration of regional anesthesia of the maxilla and mandible is achieved via the use of a dental syringe, needle, and anesthetic cartridge. Several types of dental syringes are available for use. However, the most common is the breech-loading, metallic, cartridge-type, aspirating syringe. The syringe comprises a thumb ring, finger grip, barrel containing the piston with a harpoon, and needle adaptor (Figure 3). A needle is attached to the needle adaptor, which engages the rubber diaphragm of the dental cartridge (Figure 4). The anesthetic cartridge is placed into the barrel of the syringe from the side (breech-loading). The barrel contains a piston with a harpoon that engages the rubber stopper at the end of the anesthetic cartridge (Figure 5). After the needle and cartridge have been attached, a brisk tap is given to the back of the thumb ring to ensure that the harpoon has engaged the rubber stopper at the end of the anesthetic cartridge (Figure 6).
Learn more about Equipment for Regional Anesthesia.

Figure 3. Breech-loading, metallic, cartridge-type, aspirating syringe.

Figure 4. Needle–syringe assembling. A needle is attached to the needle adaptor.
. B: A piston with a harpoon engages the rubber stopper at the end of the anesthetic cartridge while the needle adaptor engages the rubber diaphragm of the dental cartridge.")
Figure 5. A: Needle–syringe assembling. The anesthetic cartridge is placed into the barrel of the syringe from the side (breech loading). B: A piston with a harpoon engages the rubber stopper at the end of the anesthetic cartridge while the needle adaptor engages the rubber diaphragm of the dental cartridge.

Figure 6. A and B: Needle–syringe assembling. A brisk tap is given to the back of the thumb ring to ensure that the harpoon has engaged the rubber stopper at the end of the anesthetic cartridge. C: A fully loaded anesthetic syringe.
Dental needles are referred to in terms of their gauge, which corresponds to the diameter of the lumen of the needle. Increasing gauge corresponds to a smaller lumen diameter. Needles of 25 and 27 gauge are most commonly used for maxillary and mandibular regional anesthesia and are available in long and short lengths. The length of the needle is measured from the tip of the needle to the hub. The conventional long needle is approximately 40 mm in length, whereas the short needle is approximately 25 mm. Variations in needle length do exist, depending on the manufacturer.
Anesthetic cartridges are prefilled, 1.8-mL glass cylinders with a rubber stopper at one end and an aluminum cap with a diaphragm at the other end (Figure 7). The contents of an anesthetic cartridge are the local anesthetic, vasoconstrictor (anesthetic without vasoconstrictor is also available), preservative for the vasoconstrictor (sodium bisulfite), sodium chloride, and distilled water. The most common anesthetics used in clinical practice are the amide anesthetics: lidocaine and mepivacaine. Other amide anesthetics available for use are prilocaine, articaine, bupivacaine, and etidocaine. Esther anesthetics are not as commonly used but remain available. Procaine, procaine plus propoxycaine, chloroprocaine, and tetracaine are some common esther anesthetics (Table 2). Additional armamentaria include dry gauze, topical antiseptic, and anesthetic. The site of injection should be made dry with gauze, and a topical antiseptic should be used to clean the area. Topical anesthetic is applied to the area of injection to minimize discomfort during insertion of the needle into the mucous membrane (Figure 8). Common topical preparations include benzocaine, butacaine sulfate, cocaine hydrochloride, dyclonine hydrochloride, lidocaine, and tetracaine hydrochloride.

Figure 7. A: Dental cartridges. The rubber stopper is on the right end of the cartridge while the aluminum cap with the diaphragm is on the left end of the cartridge. B: Containers of dental anesthetic.
The clinician should always observe universal precautions; these include the use of protective gloves, mask, and eye protection. After withdrawing the needle when a block has been completed, the needle should always be carefully recapped to avoid accidental needle stick injury to the operator.
Retraction of the soft tissue for visualization of the injection site should be performed with the use of a dental mirror or retraction instrument. This is recommended for all maxillary and mandibular regional techniques discussed below. Use of an instrument rather than one’s fingers helps to prevent accidental needle-stick injury to the operator.
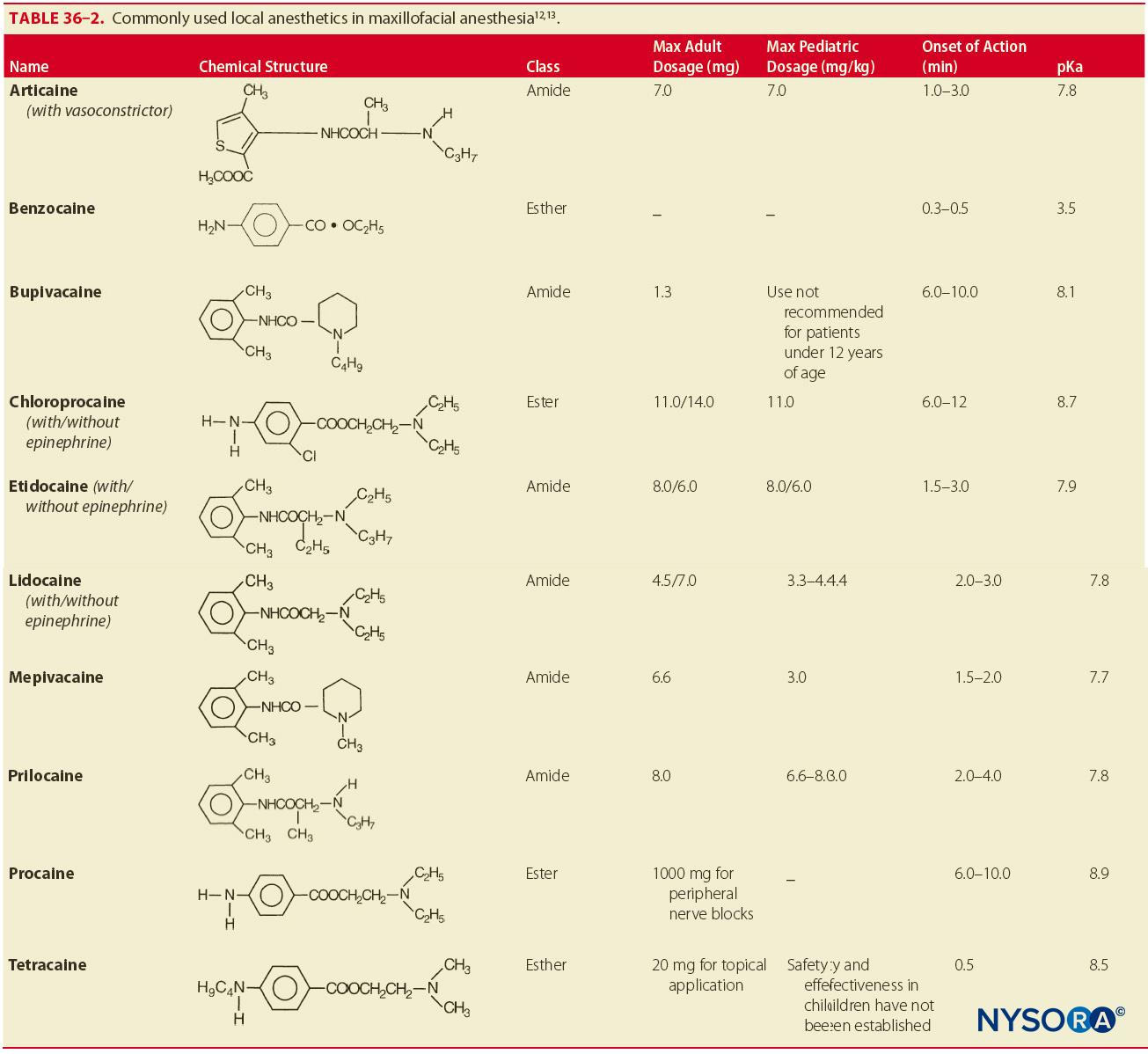

Figure 8. Topical anesthesia. Before injection, a topical anesthetic can be applied on the mucosa in the area of injection to minimize patient discomfort.
TECHNIQUES OF REGIONAL MAXILLARY ANESTHESIA
The techniques most commonly used in maxillary anesthesia include supraperiosteal (local) infiltration, periodontal ligament (intraligamentary) injection, PSA nerve block, MSA nerve block, anterior superior alveolar nerve block, greater palatine nerve block, nasopalatine nerve block, local infiltration of the palate, and intrapulpal injection (Table 3). Of less clinical application are the maxillary nerve block and intraseptal injection.
TABLE 3. Techniques of anesthesia for treatment of a localized area or one or two teeth.
| Technique | Area Anesthetized |
|---|---|
| Supraperiosteal injection | Individual teeth and buccal soft tissue |
| Periodontal ligament injection | Individual teeth and buccal soft tissue |
| Intraseptal injection | Localized soft tissue |
| Intrapulpal injection | Individual tooth |
Supraperiosteal (Local) Infiltration
The supraperiosteal, or local, infiltration is one of the simplest and most commonly used techniques for achieving anesthesia of the maxillary dentition. This technique is indicated when any individual tooth or soft tissue in a localized area is to be treated. Contraindications to this technique are the need to anesthetize multiple teeth adjacent to one another (in which case a nerve block is a preferred technique), acute inflammation and infection in the area to be anesthetized, and, less significantly, the density of bone overlying the apices of the teeth. A 25- or 27-gauge short needle is preferred for this technique.
Procedure
Identify the tooth to be anesthetized and the height of the mucobuccal fold over the tooth. This will be the injection site. The right-handed operator should stand at the 9 o’clock to 10 o’clock position, whereas the left-handed operator should stand at the 2 o’clock to 3 o’clock position. Retract the lip, and orient the syringe with the bevel toward bone. This prevents discomfort from the needle coming into contact with the bone and minimizes the risk of tearing the periosteum with the needle tip. Insert the needle at the height of the mucobuccal fold above the tooth to a depth of no more than a few millimeters, and aspirate (Figure 9). If aspiration is negative, slowly inject one-third to one-half (0.6–1.2 mL) of a cartridge of anesthetic solution over the course of 30 seconds. Withdraw the syringe, and recap the needle. Successful administration provides anesthesia to the tooth and associated soft tissue within 2–4 minutes. If adequate anesthesia has not been achieved, repeat the procedure, and deposit another one-third to one-half of the cartridge of anesthetic solution.
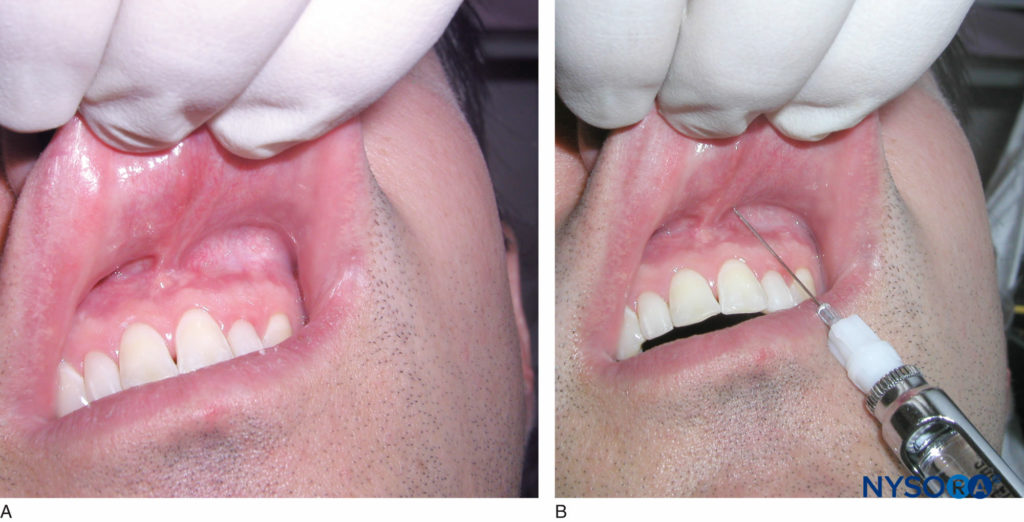
Figure 9. A: Locate the height of the mucobuccal fold over the tooth to be anesthetized. B: Clinical picture depicting a local infiltration of the maxillary left central incisor tooth. Note the penetration of the needle at the height of the mucobuccal fold above the maxillary left central incisor.
Periodontal Ligament (Intraligamentary) Injection
The periodontal ligament, or intraligamentary, injection is a useful adjunct to the supraperiosteal injection or a nerve block. Often, it is used to supplement these techniques to achieve profound anesthesia of the area to be treated. Indications for the use of the intraligamentary injection technique are the need to anesthetize an individual tooth or teeth, need for soft tissue anesthesia within the immediate vicinity of a tooth, and partial anesthesia after a field block or nerve block. A 25- or 27-gauge short needle is preferred for this technique.
Procedure
Identify the tooth or area of soft tissue to be anesthetized. The sulcus between the gingiva and the tooth is the injection site for the periodontal ligament injection. Position the patient in the supine position. For the right-handed operator, retract the lip with a retraction instrument held in the left hand, and stand where the tooth and gingiva are clearly visible. The same applies for the left-handed operator, except that the retraction instrument is held in the right hand. Hold the syringe parallel with the long axis of the tooth on the mesial or distal aspect. Insert the needle (bevel facing the root) to the depth of the gingival sulcus (Figure 10). Advance the needle until resistance is met. Then, administer a small amount of anesthetic (0.2 mL) slowly over the course of 20–30 seconds. It is normal to experience resistance to the flow of anesthetic. Successful execution of this technique provides pulpal and soft tissue anesthesia to the individual tooth or teeth to be treated.

Figure 10. Clinical picture depicting a periodontal ligament injection. Note the position of the needle between the gingival sulcus and tooth with the needle parallel to the long axis of the tooth.
Posterior Superior Alveolar Nerve Block
The PSA nerve block, otherwise known as the tuberosity block or the zygomatic block, is used to achieve anesthesia of the maxillary molar teeth up to the first molar, with the exception of its mesiobuccal root in some cases. A possible complication of this technique is the risk of hematoma formation from injection of anesthetic into the pterygoid plexus of veins or from accidental puncture of the maxillary artery. Aspiration before injection is indicated when the PSA block is given. The indications for this technique are the need to anesthetize multiple molar teeth. Anesthesia can be achieved with fewer needle penetrations than with the supraperiosteal technique, providing greater comfort to the patient. The PSA block can be given to provide anesthesia of the maxillary molars when acute inflammation and infection are present.
If inadequate anesthesia is achieved via the supraperiosteal technique, the PSA block can be used to achieve more profound anesthesia of a longer duration. The PSA block also provides anesthesia to the premolar region in a certain percentage of patients in whom the MSA is absent. Contraindications to the procedure are related to the risk of hematoma formation. In individuals with coagulation disorders, care must be taken to avoid injection into the pterygoid plexus or puncture of the maxillary artery. A short 25- or 27-gauge needle is preferred for this technique.
Procedure
Identify the height of the mucobuccal fold over the second molar. This is the injection site. The right-handed operator should stand at the 9 o’clock to 10 o’clock position, whereas the left-handed operator should stand at the 2 o’clock to 3 o’clock position. Retract the lip with a retraction instrument. Hold the syringe with the bevel toward the bone. Insert the needle at the height of the mucobuccal fold above the maxillary second molar at a 45-degree angle directed superiorly, medially, and posteriorly (one continuous movement). Advance the needle to a depth of three-fourths of its total length (Figure 11). No resistance should be felt while advancing the needle through the soft tissue. If contact is made with bone, the medial angulation is too great. Slowly retract the needle (without removing it), and bring the syringe barrel toward the occlusal plane. This allows the needle to be angulated slightly more laterally to the posterior aspect of the maxilla. Advance the needle, aspirate, and inject one cartridge of anesthetic solution slowly over the course of 1 minute, aspirating frequently during the administration.
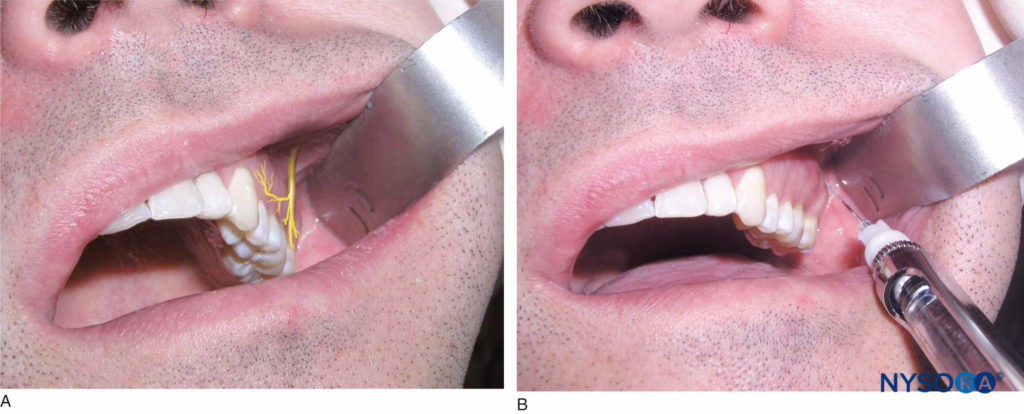
Figure 11. A: Location of the posterior superior alveolar (PSA) nerve. B: Position of the needle during the PSA nerve block. The needle is inserted at the height of the mucobuccal fold above the maxillary second molar at a 45-degree angle aimed superiorly, medially, and posteriorly.
Before injecting, one should aspirate in two planes to avoid accidental injection into the pterygoid plexus. After the first aspiration, the needle should be rotated one-quarter turn. The operator should then re-aspirate. If positive aspiration occurs, slowly retract the needle and re-aspirate in two planes. A successful injection technique results in anesthesia of the maxillary molars (with the exception of the mesiobuccal root of the first molar in some cases) and associated soft tissue on the buccal aspect.
Middle Superior Alveolar Nerve Block
The MSA nerve block is useful for procedures in which the maxillary premolar teeth or the mesiobuccal root of the first molar requires anesthesia. Although not always present it is useful if the posterior or anterior superior alveolar nerve blocks or supraperiosteal infiltration fails to achieve adequate anesthesia.
For individuals in whom the MSA nerve is absent, the PSA and anterior superior alveolar nerves provide innervation to the maxillary premolar teeth and the mesiobuccal root of the first molar. Contraindications to the procedure include acute inflammation and infection in the area of injection or a procedure involving one tooth in which local infiltration will be sufficient. A 25- or 27-gauge short needle is preferred for this technique.
Procedure
Identify the height of the mucobuccal fold above the maxillary second premolar. This is the injection site. The right-handed operator should stand at the 9 o’clock to 10 o’clock position, whereas the left-handed operator should stand at the 2 o’clock to 3 o’clock position. Retract the lip with a retraction instrument, and insert the needle until the tip is above the apex of the second premolar tooth (Figure 12). Aspirate, and inject two-thirds to one cartridge of anesthetic solution slowly over the course of 1 minute. Successful execution of this technique provides anesthesia to the pulp, surrounding soft tissue, and bone of the first and second premolar teeth and the mesiobuccal root of the first molar.

Figure 12. A: Location of the middle superior alveolar nerve. B: The needle is inserted at the height of the mucobuccal fold above the maxillary second premolar.
Anterior Superior Alveolar (Infraorbital) Nerve Block
The anterior superior alveolar, or infraorbital, nerve block, is a useful technique for achieving anesthesia of the maxillary central and lateral incisors and canine as well as the surrounding soft tissue on the buccal aspect. In patients who do not have an MSA nerve, the anterior superior alveolar nerve may also innervate the premolar teeth and mesiobuccal root of the first molar. Indications for the use of this technique include procedures involving multiple teeth and inadequate anesthesia from the supraperiosteal technique. A 25-gauge long needle is preferred for this technique.
Procedure
Place the patient in the supine position. Identify the height of the mucobuccal fold above the maxillary first premolar. This is the injection site. The right-handed operator should stand at the 10 o’clock position, whereas the left-handed operator should stand at the 2 o’clock position. Identify the infraorbital notch on the inferior orbital rim (Figure 13a). The infraorbital foramen lies just inferior to the notch, usually in line with the second premolar. Slight discomfort is felt by the patient when digital pressure is placed on the foramen. It is helpful but not necessary to mark the position of the infraorbital foramen. Retract the lip with a retraction instrument while noting the location of the foramen. Orient the bevel of the needle toward bone, and insert the needle at the height of the mucobuccal fold above the first premolar (Figure 13b).
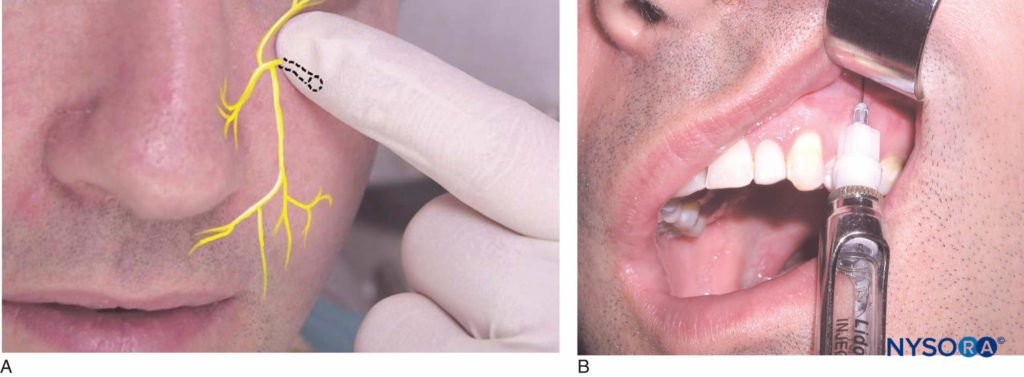
Figure 13. A: Location of the infraorbital nerve. B: The needle is kept parallel to the long axis of the maxillary first premolar and inserted at the height of the mucobuccal fold above the first premolar.
The syringe should be angled toward the infraorbital foramen and kept parallel with the long axis of the first premolar to avoid hitting the maxillary bone prematurely. The needle is advanced into the soft tissue until contact is made with the bone over the roof of the foramen. This is approximately half the length of the needle; however, length varies from individual to individual. After aspiration, approximately one-half to two-thirds (0.9–1.2 mL) of the anesthetic cartridge is deposited slowly over the course of 1 minute. It is recommended that pressure is kept over the site of injection to facilitate the diffusion of anesthetic solution into the foramen. Successful execution of this technique results in anesthesia of the lower eyelid, lateral aspect of the nose, and upper lip. Pulpal anesthesia of the maxillary central and lateral incisors, canine, buccal soft tissue, and bone is also achieved. In a certain percentage of people, the premolar teeth and the mesiobuccal root of the first molar are also anesthetized.
Greater Palatine Nerve Block
The greater palatine nerve block is useful when treatment is necessary on the palatal aspect of the maxillary premolar and molar dentition. This technique targets the area just anterior to the greater palatine canal. The greater palatine nerve exits the canal and travels forward between the bone and soft tissue of the palate.
Contraindications to this technique are acute inflammation and infection at the injection site. A 25- or 27-gauge long needle is preferred for this technique.
Procedure
The patient should be in the supine position with the chin tilted upward for visibility of the area to be anesthetized. The right-handed operator should stand at the 8 o’clock position, whereas the left-handed operator should stand at the 4 o’clock position. Using a cotton swab, locate the greater palatine foramen by placing it on the palatal tissue approximately 1 cm medial to the junction of the second and third molars (Figure 14). Although this is the usual position for the foramen, it may be located slightly anterior or posterior to this location. Gently press the swab into the tissue until the depression created by the foramen is felt.
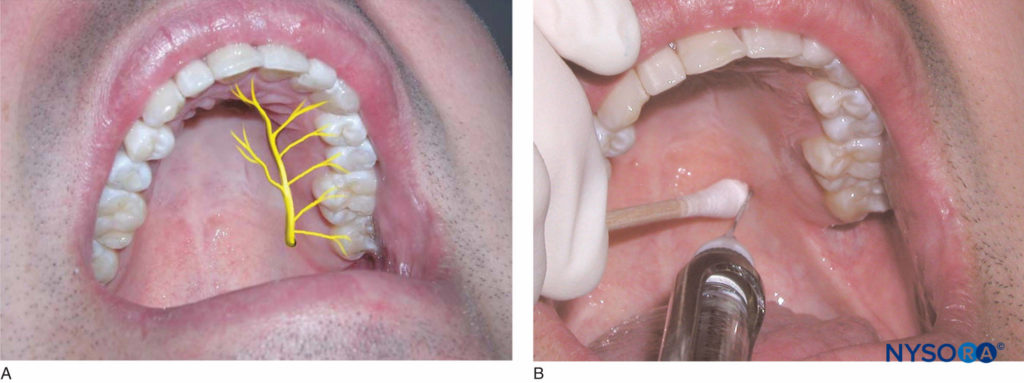
Figure 14. A: Location of the greater palatine nerve. B: The area of insertion for the greater palatine nerve block is 1 cm medial to the junction of the maxillary second and third molars.
Malamed and Trieger found that the foramen is found medial to the anterior half of the third molar approximately 50% of the time, medial to the posterior half of the second molar approximately 39% of the time, and medial to the posterior half of the third molar approximately 9% of the time. The area approximately 1–2 mm anterior to the foramen is the target injection site. Using the cotton swab, apply pressure to the area of the foramen until the tissue blanches. Aim the syringe perpendicular to the injection site, which is 1–2 mm anterior to the foramen. While keeping pressure on the foramen, inject small volumes of anesthetic solution as the needle is advanced through the tissue until contact is made with bone. The tissue will blanch in the area surrounding the injection site. Depth of penetration is usually no more than a few millimeters. Once contact is made with bone, aspirate and inject approximately one-fourth (0.45 mL) of the anesthetic solution. Resistance to deposition of anesthetic solution is normally felt by the operator. This technique provides anesthesia to the palatal mucosa and hard palate from the first premolar anteriorly to the posterior aspect of the hard palate and to the midline medially.
Nasopalatine Nerve Block
The nasopalatine nerve block, otherwise known as the incisive nerve block or sphenopalatine nerve block, anesthetizes the nasopalatine nerves bilaterally. In this technique, the anesthetic solution is deposited in the area of the incisive foramen. This technique is indicated when treatment requires anesthesia of the lingual aspect of multiple anterior teeth. A 25- or 27-gauge short needle is preferred for this technique.
Procedure
The patient should be in the supine position with the chin tilted upward for visibility of the area to be anesthetized. The right-handed operator should be at the 9 o’clock position, whereas the left-handed operator should be at the 3 o’clock position. Identify the incisive papillae. The area directly lateral to the incisive papilla is the injection site. With a cotton swab, hold pressure over the incisive papilla. Insert the needle just lateral to the papilla with the bevel against the tissue (Figure 15). Advance the needle slowly toward the incisive foramen while depositing small volumes of anesthetic and maintaining pressure on the papilla. Once contact is made with bone, retract the needle approximately 1 mm, aspirate, and inject one-fourth (0.45 mL) of a cartridge of anesthetic solution over the course of 30 seconds. Blanching of surrounding tissues and resistance to the deposition of anesthetic solution are normal. Anesthesia is provided to the soft and hard tissue of the lingual aspect of the anterior teeth from the distal of the canine on one side to the distal of the canine on the opposite side.

Figure 15. A: Location of the nasopalatine nerve. B: Needle insertion is just lateral to the incisive papilla for the nasopalatine nerve block.
Local Palatal Infiltration
The administration of local anesthetic for the palatal anesthesia of just one or two teeth is common in clinical practice. When a block is undesirable, local infiltration provides effective palatal anesthesia of the individual teeth to be treated. Contraindications include acute inflammation and infection over the area to be anesthetized. A 25- or 27-gauge short needle is preferred for this technique.
Procedure
The patient should be in the supine position with the chin tilted upward for visibility of the area to be anesthetized. Identify the area to be anesthetized. The right-handed operator should be at the 10 o’clock position, whereas the left-handed operator should be at the 2 o’clock position. The area of needle penetration is 5–10 mm palatal to the center of the crown. Apply pressure directly behind the injection site with a cotton swab. Insert the needle at a 45-degree angle to the injection site with the bevel angled toward the soft tissue (Figure 16). While maintaining pressure behind the injection site, advance the needle, and slowly deposit anesthetic solution as the soft tissue is penetrated. Advance the needle until contact is made with bone. Depth of penetration is usually no more than a few millimeters. The tissue is very firmly adherent to the underlying periosteum in this region, causing resistance to the deposition of local anesthetic. No more than 0.2–0.4 mL of anesthetic solution is necessary to provide adequate palatal anesthesia. Blanching of the tissue at the injection site immediately follows deposition of local anesthetic. Successful administration of anesthetic using this technique results in hemostasis and anesthesia of the palatal tissue in the area of injection.

Figure 16. Local infiltration on the palatal aspect of the maxillary right first premolar. The needle is inserted approximately 5–10 mm palatal to the center of the crown.
Intrapulpal Injection
Intrapulpal injection involves anesthesia of the nerve within the pulp canal of the individual tooth to be treated. When pain control cannot be achieved by any of the aforementioned methods, the intrapulpal method may be used once the pulp chamber is open. There are no contraindications to the use of this technique as it is at times the only effective method of pain control. A 25- or 27-gauge short needle is preferred for this technique.
Procedure
The patient should be in the supine position with the chin tilted upward for visibility of the area to be anesthetized. Identify the tooth to be anesthetized. The right-handed operator should be at the 10 o’clock position, whereas the left-handed operator should be at the 2 o’clock position. Assuming that the pulp chamber has been opened by an experienced dental professional, place the needle into the pulp chamber, and deposit one drop of anesthetic. Advance the needle into the pulp canal, and deposit another 0.2 mL of local anesthetic solution. It may be necessary to bend the needle in order to gain access to the chamber, especially with posterior teeth. The patient usually experiences a brief period of significant pain as the solution enters the canal, followed by immediate pain relief.
Maxillary Nerve Block
Less often used in clinical practice, the maxillary nerve block (second division block) provides anesthesia of a hemimaxilla. This technique is useful for procedures that require anesthesia of multiple teeth and surrounding buccal and palatal soft tissue in one quadrant or when acute inflammation and infection preclude successful administration of anesthesia by the forementioned methods. There are two techniques one can use to achieve the maxillary nerve block: the high tuberosity approach and the greater palatine canal approach. The high tuberosity approach carries with it the risk of hematoma formation and is therefore contraindicated in patients with coagulation disorders. The maxillary artery is the vessel of primary concern with the high tuberosity approach.
Both techniques are contraindicated when acute inflammation and infection are present over the injection site.
High Tuberosity Approach
A 25-gauge long needle is preferred for this technique. The patient should be in the supine position with the chin tilted upward for visibility of the area to be anesthetized. Identify the area to be anesthetized. The right-handed operator should be at the 10 o’clock position, whereas the left-handed operator should be at the 2 o’clock position. This technique anesthetizes the maxillary nerve as it travels through the pterygopalatine fossa. Identify the height of the mucobuccal fold just distal to the maxillary second molar. This is the injection site. The needle should enter the tissue at a 45-degree angle aimed posteriorly, superiorly, and medially, as in the PSA nerve block (Figure 11b). The bevel should be oriented toward the bone. The needle is advanced to a depth of approximately 30 mm or a few millimeters shy of the hub.
At this depth, the needle lies within the pterygopalatine fossa. The operator should then aspirate, rotate the needle one quarter turn, and aspirate again. After negative aspiration in two planes has been established, slowly inject one cartridge of anesthetic solution over the course of 1 minute. The needle is then slowly withdrawn and recapped.
Successful administration of anesthetic using the high tuberosity approach provides anesthesia to the entire hemimaxilla on the ipsilateral side of the block. This includes pulpal anesthesia to the maxillary teeth; the buccal and palatal soft tissue as far medially as the midline; and the skin of the upper lip, lateral aspect of the nose, and lower eyelid.
Greater Palatine Canal Approach
A 25-gauge long needle is preferred for this technique. Place the patient in the supine position. The right-handed operator should be at the 10 o’clock position, whereas the left-handed operator should be at the 2 o’clock position. Identify the greater palatine foramen as described in the technique for the greater palatine nerve block. The tissue directly over the greater palatine foramen is the target for injection. This technique anesthetizes the maxillary nerve as it travels through the pterygopalatine fossa via the greater palatine canal. Apply pressure to the area over the greater palatine foramen with a cotton-tipped applicator.
Administer a greater palatine nerve block using the aforementioned technique (see Figure 14b). When adequate palatal anesthesia is achieved, gently probe for the greater palatine foramen with the tip of the needle. For this technique, the syringe should be held so that the needle is aimed posteriorly. It may be necessary to change the angulation of the needle to locate the foramen.
In a case study performed by Malamed and Trieger, the majority of canals were angled 45–50 degrees. Once the foramen has been located, advance the needle to a depth of 30 mm. If resistance is met, withdraw the needle a few millimeters, and reenter at a different angle. Malamed and Trieger found bony obstructions preventing needle passage in approximately 5–15% of canals. If resistance is met early and the operator is unable to advance the needle into the canal more than a few millimeters, the procedure should be aborted and the high tuberosity approach should be considered. If no resistance is met and penetration of the canal is successful, aspirate in two planes as described above, and slowly deposit one cartridge of local anesthetic solution. As with the high tuberosity approach, the hemimaxilla on the ipsilateral side as the injection becomes anesthetized with successful execution of this technique.
Intraseptal Injection
The intraseptal technique is a useful adjunct to the aforementioned techniques (supraperiosteal, PSA, MSA, and anterior superior alveolar). Although not used as often in clinical practice, the technique offers the added advantage of hemostasis in the area of injection. Terminal nerve endings in the surrounding hard and soft tissue of individual teeth are anesthetized with this technique. Contraindications to the procedure include acute inflammation and infection over the site of injection. A 27-gauge short needle is preferred for this technique.
Procedure
Place the patient in the supine position. The target area is the interdental palpillae 2–3 mm apical to the apex of the papillary triangle (Figure 17). The right-handed operator should be at the 10 o’clock position, whereas the left-handed operator should be at the 2 o’clock position. The operator may ask the patient to turn his or her head for optimum visibility. The syringe is held at a 45-degree angle to the long axis of the tooth with the bevel facing the apex of the root. The needle is inserted into the soft tissue and is advanced until contact is made with bone. A few drops of anesthetic should be administered at this time. The needle is then advanced into the interdental septum, and 0.2 mL of anesthetic solution is deposited. Resistance to the flow of anesthetic solution is expected, and ischemia of the soft tissue surrounding the injection site ensues shortly after anesthetic solution is administered.
Table 4 lists maxillary and mandibular anesthesia techniques for the treatment of a quadrant or multiple teeth.
TABLE 4. Techniques of anesthesia for treatment of a quadrant or multiple teeth.
| Technique | Area Anesthetized |
|---|---|
| Maxillary | |
| Posterior superior alveolar nerve block | Maxillary molars (except the mesiobuccal root of the maxillary first molar in some cases), hard and soft tissue on buccal aspect |
| Middle superior alveolar nerve block | Mesiobuccal root of maxillary first molar (in some cases), premolars, and surrounding hard and soft tissue on buccal aspect |
| Anterior superior alveolar (infraorbital) nerve block | Maxillary central and lateral incisors and canine, surrounding hard and soft tissue on buccal aspect, mesiobuccal root of maxillary first molar (in some cases) |
| Greater palatine nerve block | Palatal mucosa and hard palate from first premolar anteriorly to posterior aspect of the hard palate and to midline medially |
| Nasopalatine nerve block | Hard and soft tissue of lingual aspect of maxillary anterior teeth from distal of canine on one side to distal of canine on the contralateral side |
| Maxillary nerve block | Hemimaxilla on side of injection (teeth; hard and soft, buccal, and lingual tissue) |
| Mandibular | |
| Inferior alveolar nerve block | Mandibular teeth on side of injection, buccal and lingual hard and soft tissue, lower lip |
| Buccal nerve block | Buccal soft tissue of molar region |
| Gow-Gates mandibular nerve block | Mandibular teeth to midline; hard and soft tissue of buccal and lingual aspect; anterior two-thirds of tongue; floor of mouth; skin over zygoma, posterior aspect of cheek, and temporal region on side of injection |
| Vazirani-Akinosi closed-mouth | Mandibular teeth to midline, hard and soft tissue of buccal aspect, anterior two-thirds of tongue, floor of mouth |
| Mental nerve block | Buccal soft tissue anterior to mental foramen, lower lip, chin |
| Incisive nerve block | Premolars, canine, incisors, lower lip, skin over chin, buccal soft tissue anterior to mental foramen |

Figure 17. Intraseptal technique. Note the position of the needle 3 mm apical to the apex of the papillary triangle.
TECHNIQUES OF MANDIBULAR REGIONAL ANESTHESIA
Techniques used in clinical practice for the anesthesia of the hard and soft tissues of the mandible include the supraperiosteal technique, periodontal ligament injection, intrapulpal anesthesia, intraseptal injection, inferior alveolar nerve block, long buccal nerve block, Gow-Gates technique, Vazirani-Akinosi closed-mouth mandibular block, mental nerve block, and incisive nerve block.
The supraperiosteal, periodontal ligament, intrapulpal, and intraseptal techniques are executed in the same manner as described for maxillary anesthesia. When anesthetizing the mandible, the patient should be in the semisupine or reclined position. The right-handed operator should stand at the 9 o’clock to 10 o’clock position, whereas the left-handed operator should stand at the 3 o’clock to 4 o’clock position.
Inferior Alveolar Nerve Block
The inferior alveolar nerve block is one of the most commonly used techniques in mandibular regional anesthesia. It is extremely useful when multiple teeth in one quadrant require treatment. While effective, this technique carries a high failure rate even when strict adherence to protocol is maintained. The target for this technique is the mandibular nerve as it travels along the medial aspect of the ramus before its entry into the mandibular foramen. The lingual, mental, and incisive nerves are also anesthetized. A 25-gauge long needle is preferred for this technique.
Procedure
The patient should be in the semisupine position. The righthanded operator should be in the 8 o’clock position, whereas the left-handed operator should be in the 4 o’clock position.
With the patient’s mouth open maximally, identify the coronoid notch and the pterygomandibular raphae. Three-fourths of the anteroposterior distance between these two landmarks and approximately 6–10 mm above the occlusal plane is the injection site. Use a retraction instrument to retract the cheek, and bring the needle to the injection site from the contralateral premolar region. As the needle passes through the soft tissue, deposit 1 or 2 drops of anesthetic solution. Advance the needle until contact is made with bone. Then, withdraw the needle 1 mm, and redirect the needle posteriorly by bringing the barrel of the syringe toward the occlusal plane (Figures 18a and 18b). Advance the needle to three-fourths of its depth, aspirate, and inject three-fourths of a cartridge of anesthetic solution slowly over the course of 1 minute. As the needle is withdrawn, continue to deposit the remaining one-fourth of anesthetic solution so as to anesthetize the lingual nerve (Figure 18c). Successful execution of this technique results in anesthesia of the mandibular teeth on the ipsilateral side to the midline, the associated buccal and lingual soft tissue, the lateral aspect of the tongue on the ipsilateral side, and the lower lip on the ipsilateral side.

Figure 18. A: Location of the inferior alveolar nerve. B: After making contact with bone, the needle is redirected posteriorly by bringing the barrel of the syringe toward the occlusal plane. The needle is then advanced to three-fourths of its depth. C: Location of the lingual nerve, which is anesthetized during the administration of an inferior alveolar nerve block.
Buccal Nerve Block
The buccal nerve block, otherwise known as the long buccal or buccinator block, is a useful adjunct to the inferior alveolar nerve block when manipulation of the buccal soft tissue in the mandibular molar region is indicated. The target for this technique is the buccal nerve as it passes over the anterior aspect of the ramus. Contraindications to the procedure include acute inflammation and infection over the site of injection. A 25-gauge long needle is preferred for this technique.
Procedure
The patient should be in the semisupine position. The right-handed operator should be in the 8 o’clock position, whereas the left-handed operator should be in the 4 o’clock position. Identify the most distal molar tooth on the side to be treated. The tissue just distal and buccal to the last molar tooth is the target area for injection (Figure 19). Use a retraction instrument to retract the cheek. The bevel of the needle should be toward bone, and the syringe should be held parallel with the occlusal plane on the side of the injection. The needle is inserted into the soft tissue, and a few drops of anesthetic solution are administered. The needle is advanced approximately 1–2 mm until contact is made with bone. Once contact is made with bone and aspiration is negative, 0.2 mL of local anesthetic solution is deposited. The needle is withdrawn and recapped. Successful execution of this technique results in anesthesia of the buccal soft tissue of the mandibular molar region.
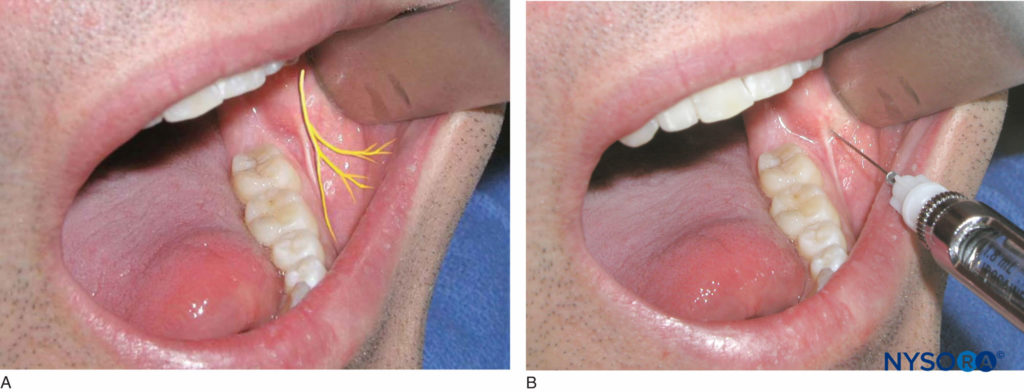
Figure 19. A: Location of the buccal nerve. B: The tissue just distal and buccal to the last molar tooth is the target area for injection.
Gow-Gates Technique
The Gow-Gates technique, or third division nerve block, is a useful alternative to the inferior alveolar nerve block and is often used when the latter fails to provide adequate anesthesia. Advantages of this technique compared with the inferior alveolar technique are its low failure rate and its low incidence of positive aspiration. The Gow-Gates technique anesthetizes the auriculotemporal, inferior alveolar, buccal, mental, incisive, mylohyoid, and lingual nerves. Contraindications include acute inflammation and infection over the site of injection and trismatic patients. A 25-gauge long needle is preferred for this technique.
Procedure
The patient should be in the semisupine position. The right-handed operator should be in the 8 o’clock position, whereas the left-handed operator should be in the 4 o’clock position. The target area for this technique is the neck of the condyle below the area of insertion of the lateral pterygoid muscle. A retraction instrument is used to retract the cheek. The patient is asked to open maximally, and the mesiolingual cusp of the maxillary second molar on the side of desired anesthesia is identified. The insertion site of the needle should be just distal to the maxillary second molar at the level of the mesiolingual cusp. Bring the needle to the insertion site in a plane that is parallel with an imaginary line drawn from the intertragic notch to the corner of the mouth on the same side as the injection (Figure 20). The orientation of the bevel of the needle is not important in this technique. Advance the needle through soft tissue approximately 25 mm until contact is made with bone. This is the neck of the condyle. Once contact is made with bone, withdraw the needle 1 mm, and aspirate. Redirect the needle superiorly, and reaspirate. If aspiration in two planes is negative, slowly inject one cartridge of local anesthetic solution over the course of 1 minute. Successful execution of this technique provides anesthesia to the ipsilateral mandibular teeth up to the midline and the associated buccal and lingual hard and soft tissue. The anterior two-thirds of the tongue; the floor of the mouth; and the skin over the zygoma, posterior aspect of the cheek, and temporal region on the ipsilateral side of injection are also anesthetized.
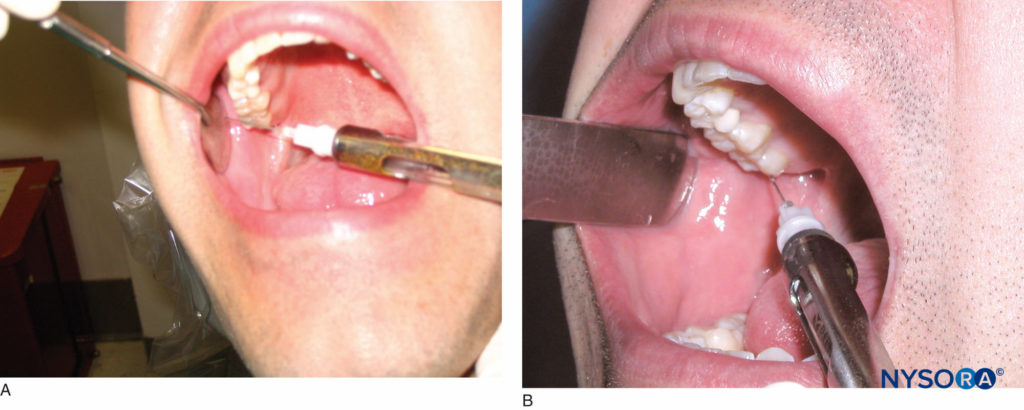
Figure 20. A: The patient is asked to open his or her mouth maximally. The mesiolingual cusp of the maxillary second molar is the reference point for the height of the injection. B: The needle is then moved distally and is held parallel to an imaginary line drawn from the intertragic notch to the corner of the mouth.
Vazirani-Akinosi Closed-Mouth Mandibular Block
The Vazirani-Akinosi closed-mouth mandibular block is a useful technique for patients with limited opening due to trismus or ankylosis of the temporomandibular joint. Limited mandibular opening precludes the administration of the inferior alveolar nerve block or use of the Gow-Gates technique, both of which require the patient to open maximally. Other advantages to this technique are the minimal risk of trauma to the inferior alveolar nerve, artery, and vein and the pterygoid muscle; a low complication rate; and minimal discomfort upon injection. Contraindications to this technique are acute inflammation and infection in the pterygomandibular space, deformity or tumor in the maxillary tuberosity region, and an inability to visualize the medial aspect of the ramus. A 25-gauge long needle is preferred for this technique.
Procedure
The patient should be in the semisupine position. The right-handed operator should be in the 8 o’clock position, whereas the left-handed operator should be in the 4 o’clock position. The gingival margin above the maxillary second and third molars and the pterygomandibular raphae serve as landmarks for this technique. A retraction instrument is used to stretch the cheek laterally. The patient should occlude gently on the posterior teeth. The needle is held parallel with the occlusal plane at the level of the gingival margin of the maxillary second and third molars. The bevel is directed away from the bone facing the midline. The needle is advanced through the mucous membrane and buccinator muscle to enter the pterygomandibular space. The needle is inserted to approximately one-half to three-fourths of its length. At this point, the needle will be in the midsection of the ptyerygomandibular space. Aspirate; if negative, one cartridge of local anesthetic solution is deposited over the course of 1 minute. Diffusion and gravitation of the local anesthetic solution anesthetizes the lingual and long buccal nerves in addition to the inferior alveolar nerve. Successful execution of this technique provides anesthesia of the ipsilateral mandibular teeth up to the midline and the associated buccal and lingual hard and soft tissue. The anterior two-thirds of the tongue and floor of the mouth are also anesthetized.
Mental Nerve Block
The mental nerve block is indicated for procedures in which manipulation of buccal soft tissue anterior to the mental foramen is necessary. Contraindications to this technique are acute inflammation and infection over the injection site. A 25- or 27-gauge short needle is preferred for this technique.
Procedure
The patient should be in the semisupine position. The righthanded operator should be in the 8 o’clock position, whereas the left-handed operator should be in the 4 o’clock position. The target area is the height of the mucobuccal fold over the mental foramen (Figures 21a and 21b). The foramen can be manually palpated by applying gentle finger pressure to the body of the mandible in the area of the premolar apices. The patient will feel slight discomfort upon palpation of the foramen. Use a retraction instrument to retract the soft tissue. The needle is directed toward the mental foramen with the bevel facing the bone. Penetrate the soft tissue to a depth of 5 mm, aspirate, and inject approximately 0.6 mL of anesthetic solution. Successful execution of this technique results in anesthesia of the buccal soft tissue anterior to the foramen, lower lip, and chin on the side of the injection.
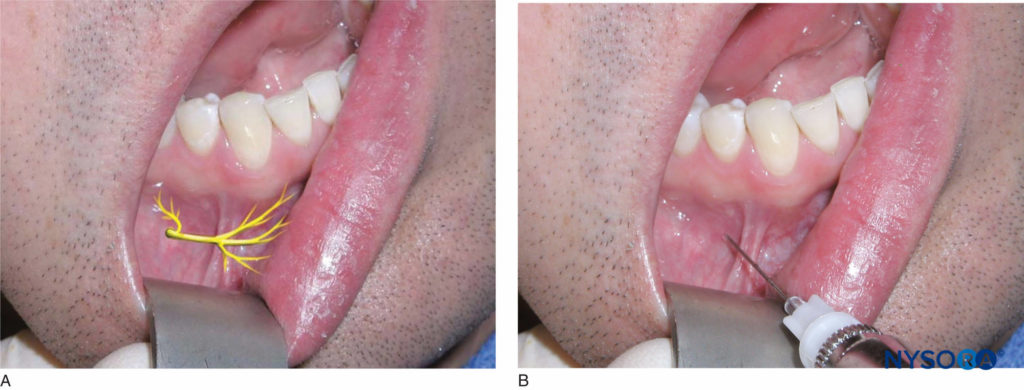
Figure 21. A: Location of the mental and incisive nerves. B: Block of the mental and incisive nerves. The needle is inserted at the height of the mucobuccal fold over the mental foramen for both the mental nerve block and the incisive nerve block.
Incisive Nerve Block
The incisive nerve block is not as frequently used in clinical practice; however, it proves very useful when treatment is limited to mandibular anterior teeth and full quadrant anesthesia is not necessary. The technique is almost identical to the mental nerve block but with one additional step. Both the mental and incisive nerves are anesthetized using this technique. Contraindications to this technique are acute inflammation and infection at the site of injection. A 25- or 27-gauge short needle is preferred for this technique.
Procedure
The patient should be in the semisupine position. The right-handed operator should be in the 8 o’clock position, whereas the left-handed operator should be in the 4 o’clock position. The target area is the height of the mucobuccal fold over the mental foramen (see Figure 21b). Identify the mental foramen as previously described. Give the patient a mental nerve block as described above, and apply digital pressure at the site of injection during administration of anesthetic solution. Continue to apply digital pressure at the site of injection 2–3 minutes after the injection is complete to aid the anesthetic in diffusing into the foramen. Successful implementation of this technique provides anesthesia to the premolars, canine, incisor teeth, lower lip, skin of the chin, and buccal soft tissue anterior to the mental foramen.
REFERENCES
- Malamed SF: Handbook of Local Anesthesia, 4th ed. Maryland Heights, MI: Mosby, 1997
- Snell RS: Clinical Anatomy for Medical Students, 5th ed. New York: Little, Brown, 1995
- Loetscher CA, Walton RE: Patterns of innervation of the maxillary first molar: a dissection study. Oral Surg Oral Med Oral Pathol 1988; 65:86–90
- McDaniel WM: Variations in nerve distributions of the maxillary teeth. J Dent Res 1956;35:916–921
- Heasman PA: Clinical anatomy of the superior alveolar nerves. Br J Oral Maxillofacial Surg 1884;22:439–447
- Malamed SF, Trieger N: Intraoral maxillary nerve block: an anatomical and clinical study. Anesthesia Progr 1983;30:44–48
- Poore TE, Carney F: Maxillary nerve block: a useful technique. J Oral Surg 1973;31:749–755
- Gow-Gates GAE: Mandibular conduction anesthesia: a new technique using extraoral landmarks. Oral Surg 1973;36:321–328
- Akinosi JO: A new approach to the mandibular nerve block. Br J Oral Maxillofacial Surg 1977;15:83–87
- Vazirani SJ: Closed mouth mandibular nerve block: a new technique. Dent Digest 1960;66:10–13