Ultrasound Pain Block Tip of the Week: Pudendal Nerve Block
A pudendal nerve block is used to diagnose and treat pudendal neuralgia, a chronic pelvic pain experienced in the regions innervated by the pudendal nerve (i.e., anterior and posterior urogenital areas) caused by repetitive activities, overuse of the pelvic floor muscles, motor vehicle accidents, falls, pelvic surgeries, radiation therapy, ischial spinal fractures, tumors, and obstetrical injuries.
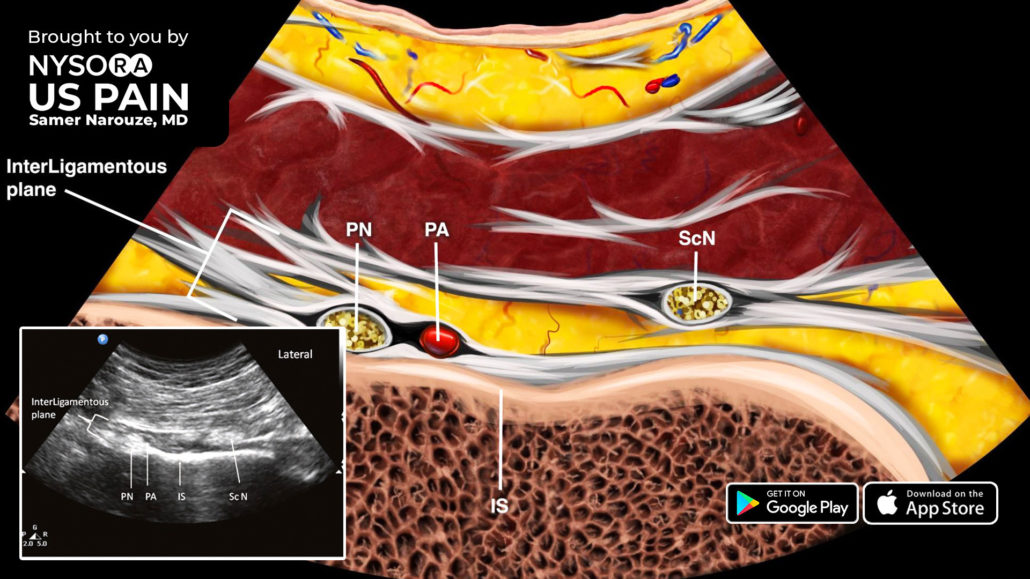
Here are 4 noticeable landmarks to help identify the level of the ischial spine right away
- The ischial spine appears as a straight, hyperechoic line, while the ischium is a curved, hyperechoic line.
- The sacrospinous ligament is visualized as a hyperechoic line lying medial to and in contact with the ischial spine.
- The piriformis muscle will disappear. Deep in the gluteus maximus muscle lies the sacrotuberous ligament, which can be easily felt as the needle advances.
The internal pudendal artery is situated on the medial portion of the ischial spine. This artery can be confirmed with the color Doppler.
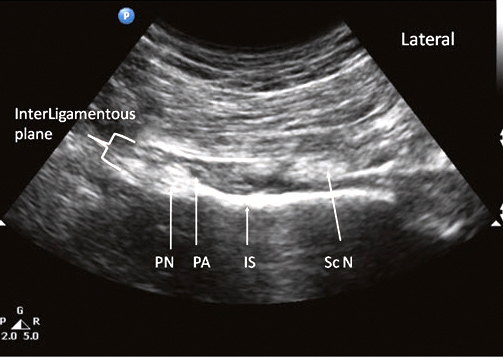 Sonoanatomy
Sonoanatomy
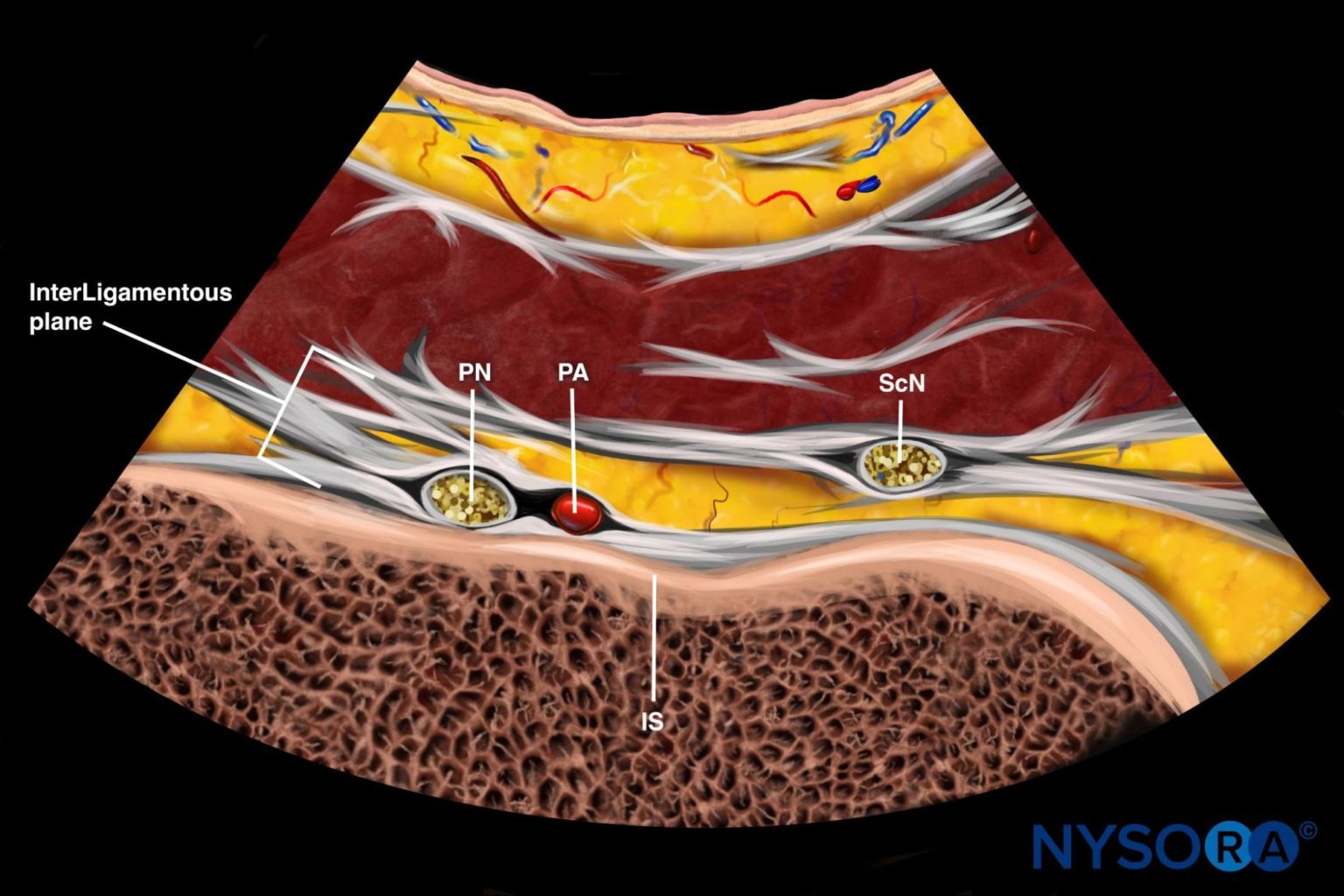
Reverse Ultrasound Anatomy
Download the US Pain App HERE to read other tips on managing acute and chronic pain and to access the complete guide to ultrasound-guided chronic pain blocks.