Tips for an Axillary Brachial Plexus Block
The most common indications for an axillary brachial plexus block include surgery of the forearm, wrist, or hand of moderate to long duration, with or without an arm tourniquet. It anesthetizes the brachial plexus at the level of the terminal branches (i.e., median, ulnar, radial, and musculocutaneous nerves), resulting in anesthesia of the upper extremity from the mid-arm down, including the hand.
Step-by-step: 3 key steps for performing an axillary brachial plexus block
- Place the transducer in a transverse orientation over the intersection of the pectoral major and biceps muscle insertion. Do not place the transducer too high in the axillary fossa.
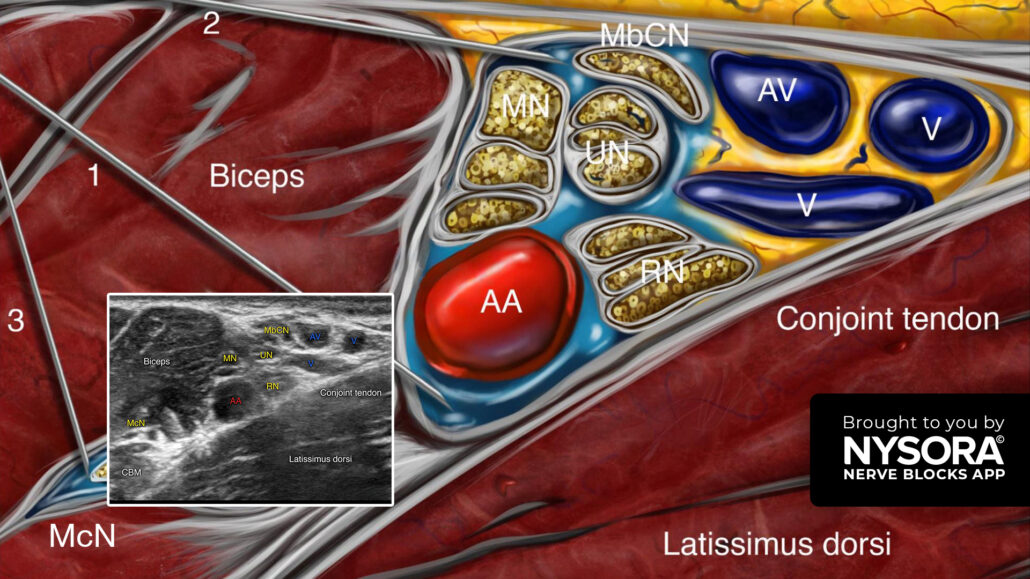
- Identify the axillary artery, the conjoint tendon, the neurovascular sheath containing the median, ulnar, and radial nerves, the muscles (i.e., biceps, coracobrachialis, and latissimus dorsi muscles), and the musculocutaneous nerve.
- Insert the needle in-plane, from lateral to medial, toward the axillary artery and inject 20 mL of local anesthetic (8 mL above the axillary artery, 8 mL below the axillary artery, and 4 mL for the musculocutaneous nerve).
Tip: When the musculocutaneous nerve travels together with the median nerve, it is not necessary to block this nerve with a separate injection.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!